Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Open access
- Published: 04 July 2022

A systematic review and meta-analysis on the association between ambient air pollution and pulmonary tuberculosis
- Christian Akem Dimala 1 , 2 &
- Benjamin Momo Kadia 3 , 4
Scientific Reports volume 12 , Article number: 11282 ( 2022 ) Cite this article
3172 Accesses
15 Citations
5 Altmetric
Metrics details
- Environmental sciences
- Health care
- Medical research
- Risk factors
There is inconclusive evidence on the association between ambient air pollution and pulmonary tuberculosis (PTB) incidence, tuberculosis-related hospital admission and mortality. This review aimed to assess the extent to which selected air pollutants are associated to PTB incidence, hospital admissions and mortality. This was a systematic review of studies published in English from January 1st, 1946, through May 31st, 2022, that quantitatively assessed the association between PM 2.5 , PM 10 , NO 2 , SO 2 , CO, O 3 and the incidence of, hospital admission or death from PTB. Medline, Embase, Scopus and The Cochrane Library were searched. Extracted data from eligible studies were analysed using STATA software. Random-effect meta-analysis was used to derive pooled adjusted risk and odds ratios. A total of 24 studies (10 time-series, 5 ecologic, 5 cohort, 2 case–control, 1 case cross-over, 1 cross-sectional) mainly from Asian countries were eligible and involved a total of 437,255 tuberculosis cases. For every 10 μg/m 3 increment in air pollutant concentration, there was a significant association between exposure to PM 2.5 (pooled aRR = 1.12, 95% CI: 1.06–1.19, p < 0.001, N = 6); PM 10 (pooled aRR = 1.06, 95% CI: 1.01–1.12, p = 0.022, N = 8); SO 2 (pooled aRR = 1.08, 95% CI: 1.04–1.12, p < 0.001, N = 9); and the incidence of PTB. There was no association between exposure to CO (pooled aRR = 1.04, 95% CI: 0.98–1.11, p = 0.211, N = 4); NO 2 (pooled aRR = 1.08, 95% CI: 0.99–1.17, p = 0.057, N = 7); O 3 (pooled aRR = 1.00, 95% CI: 0.99–1.02, p = 0.910, N = 6) and the incidence of PTB. There was no association between the investigated air pollutants and mortality or hospital admissions due to PTB. Overall quality of evidence was graded as low (GRADE approach). Exposure to PM 2.5 , PM 10 and SO 2 air pollutants was found to be associated with an increased incidence of PTB, while exposure to CO, NO 2 and O 3 was not. There was no observed association between exposure to these air pollutants and hospital admission or mortality due to PTB. The quality of the evidence generated, however, remains low. Addressing the tuberculosis epidemic by 2030 as per the 4th Sustainable Development Goal may require a more rigorous exploration of this association.
Similar content being viewed by others

Spatial patterns of lower respiratory tract infections and their association with fine particulate matter

Occupational and environmental risk factors of idiopathic pulmonary fibrosis: a systematic review and meta-analyses

Health impacts of air pollution exposure from 1990 to 2019 in 43 European countries
Introduction.
Pulmonary tuberculosis (PTB), a bacterial infection of the lungs caused by Mycobacterium tuberculosis is one of the top 10 causes of death worldwide and the leading cause of death from a single infectious agent 1 . PTB remains a global health emergency despite the significant progress that has been made worldwide in its control over the past two and a half decades 2 . Much still needs to be done to end the tuberculosis epidemic by 2030 3 as per the World Health Organisation’s (WHO) 4th sustainable development goal (SDG). This includes addressing important predisposing factors to tuberculosis infection such as smoking, diabetes, human immunodeficiency virus (HIV) and social determinants of health such as poverty, malnutrition, poor ventilation and over-crowding among others 1 , 4 . A multi-faceted and multi-sectorial approach to tuberculosis prevention, case identification, management and control of its health and social determinants is therefore required 4 , 5 .
Air pollution, currently on several global health agendas, has rapidly become a global problem with the increasing global urbanisation, transportation-related emissions, and increased energy consumption. Air pollution could therefore be an important factor to address on the journey to ending tuberculosis as there are growing concerns of its association to increased tuberculosis-related hospital admissions and deaths 6 , 7 .
There is a well-known association between different air pollutants and cardio-respiratory diseases 8 , 9 , 10 , 11 , 12 , 13 , 14 , 15 . However, there is still no conclusive evidence of an association between PTB and outdoor air pollution despite its well-known association to indoor pollution from activities such as smoking and biomass fuel burning 16 , 17 , 18 The review by Popovic et al. indicated a possible association between PM 2.5 and PTB outcomes (incidence, hospital admissions and mortality) and reported the contrasting findings from several earlier studies on the association between PM 10 , NO 2 , and SO 2 and PTB 19 , but did not synthesise these findings to determine to what extent these air pollutants are associated to PTB. Also, several studies have been published on this subject after the review by Popovic et al. This review therefore had as objectives to determine if there is an association between the selected air pollutants (PM 2.5 , PM 10 , NO 2 , SO 2 , CO, O 3 ) and PTB incidence, hospital admissions and mortality, and to what extent, by systematically reviewing and quantitatively combining published evidence on this topic.
This was a systematic literature review and meta-analysis of articles published in English from January 1st, 1946, through May 31st, 2022, that quantitatively assessed the association between ambient air pollution and PTB. The study protocol for this review was registered with the international prospective register of systematic reviews (PROSPERO) with trial registration number CRD42020165888 and has been published 20 . This review was reported according to The RepOrting standards for Systematic Evidence Syntheses (ROSES) for systematic review 21 as presented in Additional file 1 .
Deviations from the protocol
There were no deviations from the published study protocol.
Search for articles
A comprehensive search strategy (Additional file 2 ) combining medical subject headings (MeSH) and free-text searches for the appropriate keywords was developed by the authors and used to search the databases: Medline, Embase, Scopus and The Cochrane Library. The keywords ‘air pollution’, ‘carbon monoxide’, ‘nitrogen dioxide’, ‘sulphur dioxide’, ‘ozone’, and ‘particulate matter’ were combined with the keywords ‘tuberculosis’, ‘incidence’, ‘mortality’, ‘hospital admission’ and their respective synonyms, using the Boolean operator ‘AND’ in the search strategy. The search was run by the principal investigator (CAD), all searches were limited to the language English and grey literature search was not conducted given the lack of relevant studies from preliminary searches of the grey literature. Search dates of interest were January 1st, 1946, through May 31st, 2022. The search language was in English, and all the database searches were done on the same day, June 5th, 2022. The search was run twice to ensure replicability of results and the same results were obtained with each search run.
Article screening and study eligibility criteria
Screening process.
Articles returned by the search were saved on Zotero Version 5.0 reference management software and duplicates of the studies were manually removed by the principal investigator (CAD) with the assistance of the reference management software. More articles were added to the search output by the principal investigator by reviewing the reference list of relevant articles. The titles and abstracts of all the remaining articles were then independently screened for eligibility according to the set eligibility criteria by each of the two independent reviewers (CAD and BMK). The full texts of all the articles retained after the title and abstract screen, were then independently reviewed by the same two independent reviewers (CAD and BMK) for eligibility and inclusion to the analysis. The two independent reviewers compared their findings at the end of both the title and abstract screening and the full text review stages of the article selection process to ensure concordance in their final selection. There were no reviewer disagreements at all stages of the study selection process and no third reviewer to settle discordances as had been planned in the study protocol, was therefore needed due to concordance in the findings of the two independent reviewers.
Eligibility criteria
The following criteria were used during the article selection process to determine the eligible studies.
The following studies were included:
Population: Studies focused on adults aged 18 and above with PTB
Exposure: Studies that reported direct measurements on any of the air pollutants; carbon monoxide (CO), nitrogen dioxide (NO 2 ), sulphur dioxide (SO 2 ), ozone (O 3 ), particulate matter ≤ 2.5 µm (PM 2.5 ) and/or particulate matter ≤ 10 µm (PM 10 ) in any country, region, city or locality;
Outcomes: Studies that reported measures of association on the risk of PTB incidence, hospital admission and/or mortality from PTB;
Study design/Other: Cross-sectional, case–control, cohorts, case-crossover, ecological and time-series studies that reported on the association between ambient air pollution and PTB.
The following studies were excluded:
Population: Studies that reported on respiratory diseases other than PTB
Exposure: Studies that reported on other forms of air pollution such as indoor air pollution
Outcomes: Studies that reported outcomes related to PTB in combination with other respiratory diseases. Studies that reported on measures of effect/association other than risk ratios and odds ratios or that provided data from which these measures could not be calculated.
Other: Conference abstracts, editorials, letters, opinion papers, unpublished studies, same studies published in different journals with the same or a different title.
Study validity assessment
Assessment of study quality of each included study was done by both independent reviewers (CAD and BMK) using the respective Study Quality Assessment Tools of the National Health Institute/National Heart, Lung and Blood Institute (NHI/NHLBI) 22 depending on their study designs. There was no discordance in the overall rating of the quality of the eligible studies. Study quality indicators were included in the meta-regression.
The overall quality of the evidence provided by the studies with regards to the primary outcome of interest was assessed and graded as very low, low, moderate or high, using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) 23 .
Data coding and extraction strategy
Data on the publication details, study methods and outcomes of interest were extracted from the eligible studies into a Microsoft excel office 365 data extraction sheet (Additional file 3 ) by the principal investigator (CAD) and independently rechecked by a second reviewer (BMK) for accuracy. The following data were extracted: First author, year of publication, study location, study design, socio-demographic and clinical characteristics of study participants, study duration, number of tuberculosis cases and new tuberculosis cases, annual incidences of tuberculosis, mean and median concentration data on air pollutants of interest (CO, NO 2 , SO 2 , O 3 , PM 2.5 and PM 10 ), data on incidence, hospital admission and mortality from tuberculosis, including measures of effect/association (risk ratios, odds ratios and percentage change in the incidence of PTB) and their respective confidence intervals, and confounders reported by the respective studies and if studies adjusted for confounders or not. PM 2.5 and PM 10 air pollutants were measured in µg/m 3 and NO 2 , SO 2 and O 3 in parts per billion (ppb) and CO in parts per million (ppm). For studies that reported air pollutant concentrations in units other than the above, the Air Pollution Information System 24 , was used to convert air pollutant concentrations to appropriate units, taking into consideration the average yearly temperatures reported for the various cities or countries. The average annual outdoor temperature obtained from public sources was used for studies that did not report them. In studies where several measures of effect were reported for different quintiles or levels of exposure to air pollutants, the largest numerical estimates of the measures of effect were considered, to quantify the maximum extent of the association of air pollutants to PTB. When protective effects were observed among the measures of effect, the lowest numerical measures of effect were used. Default measures of effect reported by the studies were considered. Adjusted measures of effect were chosen over crude measures, and both single-pollutant models and multi-pollutant models were reported as appropriate. All data was transferred to STATA version 14.0 statistical software for analysis.
Potential effect modifiers/reasons for heterogeneity
Between-study heterogeneity was anticipated given the differences in study designs, settings, duration, sample sizes, and population characteristics based on review of existing literature.
Data synthesis and presentation
Meta-analyses were done through random effects models to account for the possibility of between-study heterogeneity. Risk ratios and odds ratios on the incidence of PTB following exposure to the selected air pollutants, and their respective confidence intervals from the various studies, were log-transformed, and the corresponding standard errors derived. Pooled summary estimates for the respective log-transformed measures of association were computed and presented on forest plots. Studies were pooled according to their study designs with ecologic studies and studies that used time-series analysis pooled together, separate from cohort and case–control studies. Heterogeneity between studies was assessed using the Cochrane’s Q test, and the I 2 test statistic was reported as a measure of the extent of this heterogeneity. The Begg’s and Egger’s statistical tests were used for the statistical assessments of publication bias and small study effect 25 , 26 . All statistical tests and plots were done on STATA version 14.0 statistical software.
Ethics approval and consent to participate
This systematic review does not require ethical approval as it entails a synthesis of data collected from several primary studies. No primary data collection from patients will be done for this systematic review.
Review descriptive statistics
Figure 1 summarises the study selection process.

PRISMA flow chart.
A total of 12,652 records were returned by the search. Following removal of duplicates, screening of titles and abstracts, addition of studies from the reference list of relevant studies, full-text reviews, 24 eligible studies were retained. Figure 1 summarises the PRISMA flow chart of the study selection process. The studies excluded following full-text review and the reasons for exclusion are presented in Additional file 4 .
Narrative synthesis including study validity assessment
Most studies were from Asian countries and a total of 437,255 tuberculosis cases were reported across the 22 studies that reported the number of tuberculosis cases over their study periods (1996–2019) 7 , 27 , 28 , 29 , 30 , 31 , 32 , 33 , 34 , 35 , 36 , 37 , 38 , 39 , 40 , 41 , 42 , 43 , 44 , 45 , 46 . Of the 24 studies included in the review, 10 were time series, 5 were cohort studies (3 retrospective, 2 prospective), 5 were ecologic, 2 were case–control studies (1 nested, 1 retrospective), 1 was a retrospective case cross-over and 1 was cross-sectional. Average male participation was at 64.9% (N = 13 studies) 7 , 27 , 29 , 30 , 31 , 32 , 33 , 34 , 35 , 37 , 40 , 43 , 46 , mean age of 46.3 years (N = 7 studies) 27 , 30 , 31 , 32 , 37 , 40 , 43 and average annual tuberculosis incidence was 45.3 per 100,000 population (N = 10 studies) 7 , 27 , 29 , 32 , 35 , 36 , 45 , 46 , 47 , 48 . Study and participant characteristics are summarised on Table 1 .
The average of the annual mean concentrations of the various air pollutants are presented on Table 2 .
Twelve studies were of good quality, eleven of fair quality and one of poor quality (Additional file 6 ). The overall quality of evidence for the association of all 6 air pollutants to the incidence of PTB was graded as low based on the study limitations affecting generalisability of the findings, and some inconsistency across the studies due to the significantly elevated between-study heterogeneity (Additional file 7 ).
Data synthesis
Association between air pollutants and pulmonary tuberculosis incidence.
There was a significant association between exposure to PM 2.5 and incidence of pulmonary tuberculosis (PTB), pooled adjusted RR = 1.12 (95% CI: 1.06–1.19), p < 0.001, N = 6, I 2 = 72.4% 7 , 29 , 38 , 39 , 43 , 49 . There was no evidence of publication bias (Begg’s test, p = 0.133 and Egger’s test, p = 0.203). Begg’s test, p = 1. Likewise, Xiong et al. 46 reported an association (RR = 3.10, 95% CI: 1.10–8.79) for a 50 µg/m 3 increase in PM 2.5 concentration. The study by Lai et al. 32 (RR = 1.39, 95% CI: 0.95–2.03) which was cohort in design did not find a significant association. Jassal et al. 28 reported an odds ratio of 25.3 (95% CI: 3.38–29.1).
There was a significant association between exposure to PM 10 and incidence of PTB, pooled adjusted RR = 1.06 (95% CI: 1.01–1.12), p = 0.022, N = 8, I 2 = 97.6% (Begg’s test, p = 0.536 and Egger’s test, p = 0.204) 7 , 29 , 35 , 39 , 40 , 43 , 44 , 49 . The studies by Lai et al. 32 (HR = 0.95, 95% CI: 0.78–1.17) and Hwang et al. 27 (male RR = 1.00, 95% CI: 0.96–1.05 and female RR = 1.01, 95% CI: 0.98–1.05) did not find a significant association. Likewise, the pooled adjusted OR was 1.03 (95% CI: 1.01–1.04), p = 0.001, N = 3, I 2 = 0% (Begg’s test, p = 1 and Egger’s test, p = 0.211) (Fig. 2 ) 31 , 34 , 37 .

Forest plot showing the individual and pooled risk ratios and odds ratios for pulmonary tuberculosis incidence for PM 2.5 and PM 10 . The dashed line on the Forest plot represents the overall pooled estimate. The grey squares and horizontal lines represent the vaccine acceptance rate of each study and their 95% confidence intervals. The size of the grey square represents the weight contributed by each study in the meta-analysis. The diamond represents the pooled vaccine acceptance rate and its 95% confidence intervals.
There was no significant association between exposure to CO and the incidence of PTB, pooled adjusted RR = 1.04 (95% CI: 0.98–1.11), p = 0.211, N = 4, I 2 = 87.4% (Begg’s test, p = 0.734 and Egger’s test, p = 0.355) 39 , 43 , 47 , 49 . The studies by Lai et al. 32 (HR = 1.89, 95% CI: 0.78–4.58) and Hwang et al. 27 (male RR = 0.99, 95% CI: 0.95–1.03 and female RR = 1.01, 95% CI: 0.98–1.04) had similar findings. The pooled adjusted OR was 1.22 (95% CI: 0.84–1.76), p = 0.305, N = 3, I 2 = 78.5% (Begg’s test, p = 1 and Egger’s test, p = 0.364) (Fig. 3 ) 31 , 34 , 37 . However, Xiong et al. 46 (RR = 1.436, 95% CI: 1.004–2.053) reported a significant association for a 100 µg/m 3 increase in CO concentration.

Forest plot showing the individual and pooled risk ratios and odds ratios for pulmonary tuberculosis incidence for CO and NO 2 . The dashed line on the Forest plot represents the overall pooled estimate. The grey squares and horizontal lines represent the odds ratios of each study and their 95% confidence intervals. The size of the grey square represents the weight contributed by each study in the meta-analysis. The diamond represents the pooled odds ratio and its 95% confidence intervals.
There was no association between exposure to NO 2 and the incidence of PTB, pooled adjusted RR = 1.08 (95% CI: 0.99–1.17), p = 0.057, N = 7, I 2 = 98% (Begg’s test, p = 1 and Egger’s test, p = 0.437) (Fig. 3 ) 7 , 35 , 39 , 40 , 43 , 48 , 49 . Lai et al. 32 (HR = 1.33, 95% CI: 1.04–1.70) found a significant association, while Hwang et al. 27 (male RR = 1.00, 95% CI: 0.96–1.05 and female RR = 1.01, 95% CI: 0.98–1.05) did not. Likewise, the pooled adjusted OR was 1.05 (95% CI: 0.95–1.17), p = 0.322, N = 3, I 2 = 72.4% (Begg’s test, p = 0.296 and Egger’s test, p = 0.145) (Fig. 3 ) 31 , 34 , 37 . However, Xiong et al. 46 (RR = 1.8, 95% CI: 1.11–2.91) reported a significant association for a 5 µg/m 3 increase in NO 2 concentration.
There was an association between exposure to SO 2 and incidence of PTB, pooled adjusted RR = 1.08 (95% CI: 1.04–1.12), p < 0.001, N = 9, I 2 = 94.4% (Begg’s test, p = 0.517 and Egger’s test, p = 0.356) (Fig. 4 ) 7 , 35 , 39 , 40 , 43 , 44 , 47 , 48 , 49 . Hwang et al. 27 (male RR = 1.07, 95% CI: 1.03–1.12 and female RR = 1.02, 95% CI: 0.98–1.07) reported similar findings in males. Likewise, Xiong et al. 46 reported an association (RR = 1.62, 95% CI: 1.12–2.33) for a 5 µg/m 3 increase in SO 2 concentration.

Forest plot showing the individual and pooled risk ratios and odds ratios for pulmonary tuberculosis incidence for SO 2 and O 3 . The dashed line on the Forest plot represents the overall pooled estimate. The grey squares and horizontal lines represent the odds ratios of each study and their 95% confidence intervals. The size of the grey square represents the weight contributed by each study in the meta-analysis. The diamond represents the pooled odds ratio and its 95% confidence intervals.
There was no significant association between O 3 exposure and incidence of PTB, pooled adjusted RR = 1.01 (95% CI: 0.97–1.06), p = 0.560, N = 4, I 2 = 75.6% (Begg’s test, p = 0.734 and Egger’s test, p = 0.734) (Fig. 4 ) 39 , 43 , 47 , 49 . While Hwang et al. 27 had similar findings (male RR = 0.99, 95% CI: 0.94–1.03 and female RR = 1.01, 95% CI: 0.97–1.05), Lai et al. 32 rather found a protective effect (HR = 0.69, 95% CI: 0.49–0.98). Xiong et al. 46 reported an association (RR = 0.96, 95% CI: 0.93–1.0) for a 5 µg/m 3 increase in O 3 concentration.
Table 3 summarises the percentage change in the number of PTB cases for the respective changes in air pollutant concentrations.
Association between air pollutants and hospital admissions and mortality due to pulmonary tuberculosis
Two studies reported a significant association between PM 2.5 and PTB mortality; OR = 1.46 (95% CI: 1.15–1.85) 33 and percentage change in cases of 0.08% (95% CI: 0.06–0.09) 45 . There was no significant association between CO, SO 2 , and O 3 and PTB mortality 47 (Table 4 ). Likewise, there was no significant association between PM 10 , CO, SO 2 , O 3 and hospital admission 30 , 47 . NO 2 was associated with hospital admission due to PTB, OR: 1.21 (95% CI: 1.10–1.33) (Table 4 ).
Subgroup analysis and meta-regression
Studies were categorised according to their duration (less than 5 years and 5 years or more), location (Asia and others), number of PTB cases (less than 5000 and 5000 or more) and study quality (good and fair/poor). None of these study characteristics could explain the observed heterogeneity across studies, except for study location with regards to exposure to PM 2.5 air pollutant. There was a higher risk of PTB incidence with PM 2.5 exposure in studies conducted out of Asia (Additional file 5 ).
Exposure to PM 2.5 , PM 10 and SO 2 air pollutants was found to be associated with an increased incidence of PTB, while exposure to CO, NO 2 and O 3 was not. There was no observed association between exposure to these air pollutants and hospital admission or mortality due to PTB. The findings of this review are particularly relevant given the increasing global concentrations and exposure to some air pollutants such as SO 2 and PM 2.5 over the past decades 50 , 51 . Public health strategies aimed at ending the tuberculosis epidemic would therefore have to work alongside interventions aimed at improving overall air quality and addressing air pollution 51 .
Air pollutants including O 3 and NO 2 mainly originate from volatile organic compounds, combustion processes including heating, power generation, the engines of vehicles and ships and also from industry emissions 52 . SO 2 originates from the burning of fossil fuels for power generation and the smelting of sulfur-containing mineral ores 52 . PM 2.5 and PM 10 which consist of particles of organic and inorganic substances are typically suspended in the air 52 . Air pollutants have been previously associated with the development of cardio-respiratory diseases in both children and adults 8 , 9 , 11 . Traffic-related pollution and several air pollutants such as O 3 , NO 2 , PM 2.5 and PM 10 , have not only been associated with exacerbations of asthma and chronic obstructive pulmonary disease, but have also been implicated in the development of these conditions especially in childhood 11 , 53 , 54 . Air pollutants are known to increase the risk of infection when inhaled as they dampen the natural defence barriers of the respiratory tract, inhibit muco-ciliary clearance, inhibit macrophages and initiate a chronic inflammatory response with the release of pro-inflammatory mediators 55 , 56 . In a similar way, exposure to particulate matter for example has immunomodulatory effects on antimycobacterial activity through impaired expression of important cytokines and chemokines which are important in controlling mycobacterial infections 57 , 58 . This reduced antimycobacterial host immune response predisposes to tuberculosis infection.
Measures and policies in various sectors such as the transport, housing and industry sectors are known to reduce air pollutions, including; prioritising walking and cycling in cities, using low-emission vehicles; using clean technologies that reduce industrial emissions; improving access to clean household energy for heating, lighting and cooking; making cities more green; using low-emission fuels and combustion-free power sources, among others 52 . In 2015, the WHO member states adopted a resolution for enhanced global response to the adverse health effects of air pollution, and the WHO has been overseeing this response through; the production of air quality guidelines and exposure limits to these air pollutants 52 .
Even though the studies by Ge et al. 59 and Xu et al. 60 reported a possible association between short-term exposure to SO 2 , our review did not assess outpatient PTB visits as an outcome. This is therefore a subject amenable to further exploration.
The studies in this review were conducted over a 24-year period and we did not observe a particular change or variation in the trend of the reported associations between exposure to the air pollutants and PTB incidence over time across the older and newer studies. Close to four fifth of the studies in our review were conducted in Asia and up to half of the studies were in China, which could affect the generalisability of the findings of this review, however, China is still a high-burden country for tuberculosis 61 , 62 . The observed between-study heterogeneity highlights the need for more uniform study designs and methods in future studies aiming to assess this association.
Interpretation of the findings from this review should take into consideration some limitations. This review did not assess the contribution of indoor air pollution and other comorbidities to the increased risk of PTB incidence, hospital admission and mortality. The different study designs and methodologies affected the types of confounders that could be adjusted for in the different studies and therefore introducing inconsistency in the adjustment of confounders across studies. This review, therefore, focused on the strongest reported associations between air pollutant exposure and PTB incidence rather than on the duration of exposure to the air pollutants.
Exposure to PM 2.5 , PM 10 , NO 2 and SO 2 air pollutants was found to be associated with an increased incidence of PTB, while exposure to CO and O 3 was not. These findings of this study and the overall quality of the evidence highlight the need for more rigorous exploration of this association.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
World Health Organization. Global Tuberculosis Report 2019 (World Health Organization, 2019).
Google Scholar
GBD Tuberculosis Collaborators. Global, regional, and national burden of tuberculosis, 1990–2016: Results from the global burden of diseases, injuries, and risk factors 2016 study. Lancet Infect Dis. 18 (12), 1329–1349 (2018).
Article Google Scholar
United Nations. Sustainable Development Goals. Goal 3: Ensure healthy lives and promote well-being for all at all ages [Internet]. https://www.un.org/sustainabledevelopment/health/ [cited 2020 Jan 17].
Hargreaves, J. R. et al. The social determinants of tuberculosis: From evidence to action. Am. J. Public Health 101 (4), 654–662 (2011).
Article PubMed PubMed Central Google Scholar
Grobusch, M. P. & Kapata, N. Global burden of tuberculosis: Where we are and what to do. Lancet Infect. Dis. 18 (12), 1291–1293 (2018).
Article PubMed Google Scholar
Rajaei, E. et al. Outdoor air pollution affects tuberculosis development based on geographical information system modeling. Biomed. Biotechnol. Res. J. BBRJ 2 (1), 39 (2018).
Li, Z. et al. Long-term effect of exposure to ambient air pollution on the risk of active tuberculosis. Int. J. Infect. Dis. 1 (87), 177–184 (2019).
Article CAS Google Scholar
Requia, W. J. et al. Global association of air pollution and cardiorespiratory diseases: A systematic review, meta-analysis, and investigation of modifier variables. Am. J. Public Health 108 (S2), S123–S130 (2017).
Atkinson, R. W., Kang, S., Anderson, H. R., Mills, I. C. & Walton, H. A. Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: A systematic review and meta-analysis. Thorax 69 (7), 660–665 (2014).
Article CAS PubMed Google Scholar
Ab Manan, N., Noor Aizuddin, A. & Hod, R. Effect of air pollution and hospital admission: A systematic review. Ann. Glob. Health 84 (4), 670–678 (2018).
Kelly, F. J. & Fussell, J. C. Air pollution and airway disease. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 41 (8), 1059–1071 (2011).
Moore, E. et al. Global associations between air pollutants and chronic obstructive pulmonary disease hospitalizations. A systematic review. Ann. Am. Thorac. Soc. 13 (10), 1814–1827 (2016).
PubMed PubMed Central Google Scholar
Song, Q., Christiani, D. C., Wang, X. & Ren, J. The global contribution of outdoor air pollution to the incidence, prevalence, mortality and hospital admission for chronic obstructive pulmonary disease: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 11 (11), 11822–11832 (2014).
Schwartz, J. PM10 ozone, and hospital admissions for the elderly in Minneapolis-St. Paul, Minnesota. Arch. Environ. Health Int. J. 49 (5), 366–374 (1994).
Dockery, D. W. et al. Effects of inhalable particles on respiratory health of children. Am. Rev. Respir. Dis. 139 (3), 587–594 (1989).
Sumpter, C. & Chandramohan, D. Systematic review and meta-analysis of the associations between indoor air pollution and tuberculosis. Trop. Med. Int. Health 18 (1), 101–108 (2013).
Kolappan, C. & Subramani, R. Association between biomass fuel and pulmonary tuberculosis: A nested case–control study. Thorax 64 (8), 705–708 (2009).
Kurmi, O. P., Sadhra, C. S., Ayres, J. G. & Sadhra, S. S. Tuberculosis risk from exposure to solid fuel smoke: A systematic review and meta-analysis. J. Epidemiol. Community Health 68 (12), 1112–1118 (2014).
Popovic, I. et al. A systematic literature review and critical appraisal of epidemiological studies on outdoor air pollution and tuberculosis outcomes. Environ. Res. 170 , 33–45 (2019).
Dimala, C. A., Kadia, B. M. & Hansell, A. The association between ambient air pollution and pulmonary tuberculosis: A systematic review protocol. Environ. Evid. 9 (1), 29 (2020).
Haddaway, N. R., Macura, B., Whaley, P. & Pullin, A. S. ROSES RepOrting standards for Systematic Evidence Syntheses: Pro forma, flow-diagram and descriptive summary of the plan and conduct of environmental systematic reviews and systematic maps. Environ. Evid. 7 (1), 7 (2018).
Study Quality Assessment Tools—NHLBI, NIH [Internet]. https://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools [cited 2017 Nov 2].
What is GRADE?—BMJ Best Practice [Internet]. https://bestpractice.bmj.com/info/toolkit/learn-ebm/what-is-grade/ [cited 2020 Jan 17].
Unit Conversion | Air Pollution Information System [Internet]. http://www.apis.ac.uk/unit-conversion [cited 2020 Feb 10].
Begg, C. B. & Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 50 (4), 1088–1101 (1994).
Article CAS PubMed MATH Google Scholar
Egger, M., Smith, G. D., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 315 (7109), 629–634 (1997).
Article CAS PubMed PubMed Central Google Scholar
Hwang, S. et al. Impact of outdoor air pollution on the incidence of tuberculosis in the Seoul metropolitan area, South Korea. Korean J. Intern. Med. 29 (2), 183–190 (2014).
Jassal, M. S., Bakman, I. & Jones, B. Correlation of ambient pollution levels and heavily-trafficked roadway proximity on the prevalence of smear-positive tuberculosis. Public Health 127 (3), 268–274 (2013).
Smith, G. S., Schoenbach, V. J., Richardson, D. B. & Gammon, M. D. Particulate air pollution and susceptibility to the development of pulmonary tuberculosis disease in North Carolina: An ecological study. Int. J. Environ. Health Res. 24 (2), 103–112 (2014).
Álvaro-Meca, A., Díaz, A., de Miguel, D. J., Resino, R. & Resino, S. Environmental factors related to pulmonary tuberculosis in HIV-infected patients in the combined antiretroviral therapy (cART) era. PLoS One 11 (11), e0165944 (2016).
Article PubMed PubMed Central CAS Google Scholar
Chen, K. Y. et al. Particulate matter is associated with sputum culture conversion in patients with culture-positive tuberculosis. Ther. Clin. Risk Manag. 12 , 41 (2016).
Lai, T. C. et al. Ambient air pollution and risk of tuberculosis: A cohort study. Occup. Environ. Med. 73 (1), 56–61 (2016).
Peng, Z., Liu, C., Xu, B., Kan, H. & Wang, W. Long-term exposure to ambient air pollution and mortality in a Chinese tuberculosis cohort. Sci. Total Environ. 15 (580), 1483–1488 (2017).
Article ADS CAS Google Scholar
Smith Geneé, S. et al. Air pollution and pulmonary tuberculosis: A nested case-control study among members of a Northern California Health Plan. Environ. Health Perspect. 124 (6), 761–768 (2016).
Zhu, S. et al. Ambient air pollutants are associated with newly diagnosed tuberculosis: A time-series study in Chengdu, China. Sci Total Environ. 631–632 , 47–55 (2018).
Article ADS PubMed CAS Google Scholar
Joob, B. & Wiwanitkit, V. Incidence of pulmonary tuberculosis and particulate matter 2.5 pollutant level: The association analysis for 2019 air pollution Crisis, Bangkok, Thailand. Biomed. Biotechnol. Res. J. 3 (2), 126–126 (2019).
Yao, L. et al. Ambient air pollution exposures and risk of drug-resistant tuberculosis. Environ. Int. 124 , 161–169 (2019).
Article PubMed CAS Google Scholar
Carrasco-Escobar, G., Schwalb, A., Tello-Lizarraga, K., Vega-Guerovich, P. & Ugarte-Gil, C. Spatio-temporal co-occurrence of hotspots of tuberculosis, poverty and air pollution in Lima, Peru. Infect. Dis. Poverty 9 (1), 32 (2020).
Huang, K. et al. Association between short-term exposure to ambient air pollutants and the risk of tuberculosis outpatient visits: A time-series study in Hefei, China. Environ. Res. 184 , 109343 (2020).
Wang, W. et al. Epidemiological characteristics of tuberculosis and effects of meteorological factors and air pollutants on tuberculosis in Shijiazhuang, China: A distribution lag non-linear analysis. Environ. Res. 22 , 110310 (2020).
Yang, J. et al. A study on the relationship between air pollution and pulmonary tuberculosis based on the general additive model in Wulumuqi, China. Int. J. Infect. Dis. 1 (96), 42–47 (2020).
You, S., Tong, Y. W., Neoh, K. G., Dai, Y. & Wang, C. H. On the association between outdoor PM2.5 concentration and the seasonality of tuberculosis for Beijing and Hong Kong. Environ. Pollut. Barking Essex 2016 (218), 1170–1179 (1987).
Liu, Y., Cui, L. L., Hou, L. J., Yu, C. B., Tao, N. N., Liu, J. Y. et al . Ambient air pollution exposures and newly diagnosed pulmonary tuberculosis in Jinan, China: A time series study. Sci. Rep. [ Internet ] 8 (1). https://www.scopus.com/inward/record.uri?eid=2-s2.0-85057222564&doi=10.1038%2fs41598-018-35411-6&partnerID=40&md5=688c7ce37da23c36a007e125ddddadbc (2018).
Kim, H., Yu, S. & Choi, H. Effects of particulate air pollution on tuberculosis development in seven major cities of Korea from 2010 to 2016: Methodological considerations involving long-term exposure and time lag. Epidemiol. Health 42 , e2020012 (2020).
Liu, Y. et al. Effect of ambient air pollution on tuberculosis risks and mortality in Shandong, China: A multi-city modeling study of the short- and long-term effects of pollutants. Environ. Sci. Pollut. Res. Int. 28 (22), 27757–27768 (2021).
Xiong, Y. et al. Association of daily exposure to air pollutants with the risk of tuberculosis in Xuhui District of Shanghai, China. Int. J. Environ. Res. Public Health 19 (10), 6085 (2022).
Sohn, M. et al. Association of social deprivation and outdoor air pollution with pulmonary tuberculosis in spatiotemporal analysis. Int. J. Environ. Health Res. 29 (6), 657–667 (2019).
Liu, F., Zhang, Z., Chen, H. & Nie, S. Associations of ambient air pollutants with regional pulmonary tuberculosis incidence in the central Chinese province of Hubei: A Bayesian spatial-temporal analysis. Environ. Health 19 (1), 51 (2020).
Wang, H., Tian, C., Wang, W. & Luo, X. Temporal cross-correlations between ambient air pollutants and seasonality of tuberculosis: A time-series analysis. Int. J. Environ. Res. Public Health [ Internet ] 16 (9). https://www.scopus.com/inward/record.uri?eid=2-s2.0-85065795216&doi=10.3390%2fijerph16091585&partnerID=40&md5=6b4fa1102eabb1f409e8770c89f3a35f (2019).
Butt, E. W. et al. Global and regional trends in particulate air pollution and attributable health burden over the past 50 years. Environ. Res. Lett. 12 (10), 104017 (2017).
Shaddick, G., Thomas, M. L., Mudu, P., Ruggeri, G. & Gumy, S. Half the world’s population are exposed to increasing air pollution. Npj Clim. Atmos. Sci. 3 (1), 1–5 (2020).
Ambient (outdoor) air pollution [Internet]. https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health [cited 2022 Jun 11].
McConnell, R. et al. Asthma in exercising children exposed to ozone: A cohort study. Lancet Lond. Engl. 359 (9304), 386–391 (2002).
Gauderman, W. J. et al. The effect of air pollution on lung development from 10 to 18 years of age. N. Engl. J. Med. 351 (11), 1057–1067 (2004).
Gasser, M. et al. Toxic effects of brake wear particles on epithelial lung cells in vitro. Part Fibre Toxicol. 6 (1), 30 (2009).
Behndig, A. F. et al. Airway antioxidant and inflammatory responses to diesel exhaust exposure in healthy humans. Eur. Respir. J. 27 (2), 359–365 (2006).
Article ADS CAS PubMed Google Scholar
Rivas, C. E., Cantarella, P., Sarkar, S., Rockafellow, M., Osornio Vargas, A. R., Torres, M. et al . Particulate air pollution matter (PM) modifies innate immunity of type II pneumocytes (A549) against mycobacterium tuberculosis. Am. J. Respir. Crit. Care Med . [ Internet ]. 189 , Meeting Abstracts. https://doi.org/10.1164/ajrccm-conference.2014.189.1_MeetingAbstracts.A2489 (2014).
Sarkar, S. et al. Suppression of the NF-κB pathway by diesel exhaust particles impairs human antimycobacterial immunity. J. Immunol. 188 (6), 2778–2793 (2012).
Ge, E. et al. Ambient sulfur dioxide levels associated with reduced risk of initial outpatient visits for tuberculosis: A population based time series analysis. Environ. Pollut. 228 , 408–415 (2017).
Xu, M. et al. Association of air pollution with the risk of initial outpatient visits for tuberculosis in Wuhan, China. Occup. Environ. Med. 76 (8), 560–566 (2019).
Tuberculosis (TB) [Internet]. https://www.who.int/news-room/fact-sheets/detail/tuberculosis [cited 2021 Apr 3].
Tuberculosis China [Internet]. https://www.who.int/westernpacific/health-topics/tuberculosis [cited 2021 Apr 3].
Download references
Author information
Authors and affiliations.
Health and Human Development (2HD) Research Network, Douala, Cameroon
Christian Akem Dimala
Department of Medicine, Reading Hospital, Tower Health System, West Reading, PA, USA
Health Education and Research Organisation (HERO) Cameroon, Buea, Cameroon
Benjamin Momo Kadia
Department of Clinical Sciences, Liverpool School of Tropical Medicine, Liverpool, UK
You can also search for this author in PubMed Google Scholar
Contributions
C.A.D. conceived and designed the experiments. C.A.D. and B.M.K. conducted the experiments. C.A.D. produced the manuscript. B.M.K. reviewed the manuscript. All authors approved the final copy of the manuscript.
Corresponding author
Correspondence to Benjamin Momo Kadia .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary information 1., supplementary information 2., supplementary information 3., supplementary information 4., supplementary information 5., supplementary information 6., supplementary information 7., supplementary information 8., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Dimala, C.A., Kadia, B.M. A systematic review and meta-analysis on the association between ambient air pollution and pulmonary tuberculosis. Sci Rep 12 , 11282 (2022). https://doi.org/10.1038/s41598-022-15443-9
Download citation
Received : 21 December 2021
Accepted : 23 June 2022
Published : 04 July 2022
DOI : https://doi.org/10.1038/s41598-022-15443-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
This article is cited by
The effects of meteorological factors and air pollutants on the incidence of tuberculosis in people living with hiv/aids in subtropical guangxi, china.
- Fengyi Wang
- Zongxiang Yuan
BMC Public Health (2024)
By submitting a comment you agree to abide by our Terms and Community Guidelines . If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.

Click through the PLOS taxonomy to find articles in your field.
For more information about PLOS Subject Areas, click here .
Loading metrics
Open Access
Peer-reviewed
Research Article
The effect of air-pollution and weather exposure on mortality and hospital admission and implications for further research: A systematic scoping review
Roles Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Visualization, Writing – original draft, Writing – review & editing
* E-mail: [email protected]
Affiliation School of Geography and Sustainable Development, University of St Andrews, Scotland, United Kingdom
Roles Conceptualization, Funding acquisition, Supervision, Writing – review & editing
Affiliation School of Medicine, University of St Andrews, Scotland, United Kingdom
Roles Methodology, Validation
Affiliation Department of Landscape Design and Ecosystem Management, American University of Beirut, Beirut, Lebanon
Roles Conceptualization, Funding acquisition, Investigation, Supervision, Writing – review & editing
- Mary Abed Al Ahad,
- Frank Sullivan,
- Urška Demšar,
- Maya Melhem,
- Published: October 29, 2020
- https://doi.org/10.1371/journal.pone.0241415
- Peer Review
- Reader Comments
Air-pollution and weather exposure beyond certain thresholds have serious effects on public health. Yet, there is lack of information on wider aspects including the role of some effect modifiers and the interaction between air-pollution and weather. This article aims at a comprehensive review and narrative summary of literature on the association of air-pollution and weather with mortality and hospital admissions; and to highlight literature gaps that require further research.
We conducted a scoping literature review. The search on two databases (PubMed and Web-of-Science) from 2012 to 2020 using three conceptual categories of “environmental factors”, “health outcomes”, and “Geographical region” revealed a total of 951 records. The narrative synthesis included all original studies with time-series, cohort, or case cross-over design; with ambient air-pollution and/or weather exposure; and mortality and/or hospital admission outcomes.
The final review included 112 articles from which 70 involved mortality, 30 hospital admission, and 12 studies included both outcomes. Air-pollution was shown to act consistently as risk factor for all-causes, cardiovascular, respiratory, cerebrovascular and cancer mortality and hospital admissions. Hot and cold temperature was a risk factor for wide range of cardiovascular, respiratory, and psychiatric illness; yet, in few studies, the increase in temperature reduced the risk of hospital admissions for pulmonary embolism, angina pectoris, chest, and ischemic heart diseases. The role of effect modification in the included studies was investigated in terms of gender, age, and season but not in terms of ethnicity.
Air-pollution and weather exposure beyond certain thresholds affect human health negatively. Effect modification of important socio-demographics such as ethnicity and the interaction between air-pollution and weather is often missed in the literature. Our findings highlight the need of further research in the area of health behaviour and mortality in relation to air-pollution and weather, to guide effective environmental health precautionary measures planning.
Citation: Abed Al Ahad M, Sullivan F, Demšar U, Melhem M, Kulu H (2020) The effect of air-pollution and weather exposure on mortality and hospital admission and implications for further research: A systematic scoping review. PLoS ONE 15(10): e0241415. https://doi.org/10.1371/journal.pone.0241415
Editor: Chon-Lin Lee, National Sun Yat-sen University, TAIWAN
Received: June 23, 2020; Accepted: October 15, 2020; Published: October 29, 2020
Copyright: © 2020 Abed Al Ahad et al. This is an open access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: All relevant data are within the paper and its Supporting Information files.
Funding: This review is part of a PhD project that is funded by the St Leonard’s PhD scholarship, University of St Andrews, Scotland, United Kingdom. The open access publication fees were funded by the University of St Andrews Libraries, Scotland, United Kingdom.
Competing interests: The authors declare that they have no conflict of interest.
Introduction
Air-pollution and weather exposure beyond region-specific thresholds have serious effects on the public health [ 1 , 2 ]. Worldwide, population growth, increased urbanization, economic and industrial growth, intense energy consumption, high usage of transportation vehicles, improved living standards, and changing lifestyles and consumption patterns for at least the last 100 years have resulted in increased emissions of air pollutants including greenhouse gases; and fluctuations in ambient temperature and other weather variables [ 3 , 4 ].
Ambient air-pollution consists of a range of pollutants including particulate matters with diameters of less than 10 μm (PM10) and less than 2.5 μm (PM2.5), nitrogen oxides (NOx) including nitrogen dioxide (NO2), Sulphur dioxide (SO2), Carbon monoxide (CO), and Ozone (O3) that have been associated with a range of different acute and chronic health conditions [ 5 , 6 ].
Weather exposure in terms of changing temperature, relative humidity, rainfall and other weather patterns can cause a wide range of acute illness and result in deaths especially among vulnerable populations who lack adequate physiological and behavioural responses to weather fluctuations [ 7 , 8 ]. Age (elderly and children vs adults), sex, socioeconomic factors (poverty, education, and ethnicity among others), pre-existing chronic diseases, use of certain medications, and environmental conditions such as the absence of central heating increase individual’s susceptibility to environmental exposures [ 1 , 9 , 10 ]. Research has shown that hospital admissions and mortality increase when weather exposure exceed certain thresholds with lags up to 20 days [ 11 – 14 ].
Most of the literature has shown positive correlations of air-pollution and/or exposure to weather variables beyond region-specific thresholds with all-cause and cause-specific mortality and/or hospital admission especially related to respiratory and cardiovascular diseases [ 14 – 21 ]. Though, there is a lack of information on wider aspects including the role of some effect modifiers such as ethnicity and the interaction between air-pollution and weather factors. Literature has shown that ethnic minorities often live in more disadvantaged, highly populated urban communities with poor housing conditions and higher levels of air pollution exposure [ 22 – 24 ]. This results in poorer health and higher risk for chronic health problems with time. Similar to ethnicity, the interaction between air-pollution and weather variables in relation to health outcomes is often missed in the literature despite its importance in minimizing biased estimations. Air pollutants are highly reactive, and their formation is either catalysed or slowed down based on the existing weather conditions. For example, the presence of sunlight catalyses the formation of ozone pollutant resulting in higher ozone concentrations during the summer [ 25 ].
In this context, a thorough literature review is needed to map the available literature and highlight areas that require further research and investigation. Not to mention that further understanding of the effect of air-pollution and weather exposure on mortality and hospital admission is needed to achieve better environmental and health system planning, organization, resources allocation, and interventions. This article aims to provide a comprehensive review and narrative summary (not numerical estimate) of literature on the association of air-pollution and weather with mortality and hospital admissions; and to shed the light on areas that require further research. As far as we are aware, this is the first literature review examining the effect of multiple exposures (air-pollution and weather) on multiple outcomes (mortality and hospital admissions). We chose to focus our scoping literature review on countries that are part of the single European Union (EU) market (Austria, Belgium, Bulgaria, Croatia, Republic of Cyprus, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain and Sweden, Norway, and Switzerland) and United Kingdom (UK) because these countries exhibit similar socio-economic, environmental, and health policies; minimizing the contextual differences in the effect of air-pollution and weather on mortality and hospital admission. Literature examining the effect of air-pollution and/or weather on mortality and hospital admissions in countries outside the EU and UK will be used for comparison purposes.
Materials and methods
Search strategy and database sources.
To ensure methodological reliability, we carried out our scoping literature review according to the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses for scoping reviews” (PRISMA-ScR) guidelines ( S1 Checklist ) [ 26 ].
A literature search was performed on the 6 th of February 2020 using “PubMed” and “Web of Science” database sources that cover health, medical, and environmental literature. We attempted to assess the effects of air-pollution and weather events on mortality and hospital admission in Europe by searching original research articles published in peer-reviewed journals in the last 8 years (between 06/02/2012 and 06/02/2020 inclusive). We chose to review research published in the last 8 years because in March 2007, the European Union (EU) Heads of State and Government endorsed an “integrated climate change and energy strategy” that will come into action post the expiry of Kyoto Protocol targets in 2012 and that aims to combat climate change and weather fluctuations and cut air-pollution emissions to 30% below the 1990 levels [ 27 ].
Our search strategy was divided into three conceptual categories: “environmental factors”, “health outcomes”, and “Geographical region”. The “Environmental factors” refers to air-pollution, including PM10, PM2.5, NO2, SO2, CO, and O3 air pollutants and to weather variables, including air temperature, rainfall, wind, relative humidity, and vapour pressure. The “health outcomes” include hospital admissions and mortality and the “Geographical region” refers to the EU countries and UK. For each conceptual category, a set of “MeSH” and “All Fields” terms joined by the Boolean operator “OR” were developed. Later, the three conceptual categories’ search terms were joined using the Boolean operator “AND”. Our search strategy excluded the “influenza infections”, as these are considered confounders rather than outcomes for air-pollution and weather exposure. For more details about the search codes used to navigate PubMed and Web of Science search engines, please refer to S1 Table .
To minimize finding irrelevant literature, our search was limited to the following categories in the “Web of Science” search engine: environmental sciences, public environmental occupational health, medicine general internal, environmental studies, multidisciplinary sciences, geosciences multidisciplinary, respiratory system, geography physical, geography, cardiac cardiovascular systems, urban studies, healthcare sciences services, peripheral vascular disease, medicine research experimental, emergency medicine, critical care medicine, health policy services, primary healthcare, social sciences biomedical, and demography. Grey literature, non-English language articles, conference abstracts, books, reports, masters and PhD dissertations, and unpublished studies were excluded from this review.
Inclusion and exclusion criteria
To determine the studies that would be included in this scoping review, a set of inclusion and exclusion criteria were developed for the procedure of title, keyword, and abstract screening.
The inclusion criteria involved original quantitative research studies conducted in the EU and UK; that included at least one analysis where mortality and/or hospital admission was the outcome and where one or more of the following exposures were investigated: 1) ambient air pollutants including PM10, PM2.5, CO, NO2/NOx, SO2, and O3; 2) weather exposures including temperature, rainfall, wind, humidity, and pressure; and 3) extreme weather events including heat waves, cold spells, and droughts. Due to the large amount of literature on this topic and to allow comparable results between the studies, this review was limited to cohort, time-series, and case-crossover/self-controlled quantitative study designs where hazard ratios (HR), relative risks (RR), odd ratios (OR), or percentage increase were reported for quantifying the factors associated with mortality and hospital admission. These three study designs allow a temporal follow up to evaluate the effect of time varying exposures (air-pollution and weather) on the mortality and hospital admission health outcomes.
The exclusion criteria included the following:
- Methodological studies
- Original data studies that investigated the effect of ambient air-pollution and/or weather on mortality and/or hospital admission in countries outside the EU market and UK
- Articles studying the effect of indoor air-pollution on mortality and hospital admission
- Studies examining air-pollution and weather exposure on animals and plants
- Studies on occupational air-pollution exposure
- Non-English language articles
- Mortality and/or hospital admission projections and forecasting studies
- Protocol and letter to editor papers
- Qualitative research studies
- All types of literature reviews including but not limited to narrative, scoping, and systematic literature reviews
Screening and data abstraction
Our search strategy revealed 487 articles from the “PubMed” database and 517 articles from the “Web of Science” database. These articles were exported to the citation manager software “Endnote” where 53 duplicates were identified and removed resulting in a total of 951 articles ( Fig 1 ). Using the titles, key words, and abstracts, the 951 articles were screened for relevance according to the inclusion and exclusion criteria, explained in the previous section only by first author (MA). To ensure a rigorous and reliable application of the inclusion and exclusion criteria in the screening process, a second researcher (MM) screened independently a sample of 20% of the titles and abstracts of the 951 identified records. Disagreements between the two researchers were resolved through discussion until consensus was reached. All the studies that met the inclusion criteria (n = 149 articles) were retrieved for full text screening by MA. Following the full text screening phase, an additional 37 articles were excluded by MA resulting in a total of 112 articles to be included in the final narrative synthesis ( Fig 1 ).
- PPT PowerPoint slide
- PNG larger image
- TIFF original image
https://doi.org/10.1371/journal.pone.0241415.g001
For narrative synthesis, the following information was retrieved from the 112 articles:
- Study design
- Location of the study population
- The outcome of interest
- Sample size
- Exposure variables
- The confounders adjusted for
- The assessed exposure time and the lags considered
- The exposure assessment method
- The statistical/modelling approach
- The relative risks (RR)/incident relative risks (IRR)/odd ratios (OR)/hazard ratios (HR) with their respective confidence intervals or the percentage increase that quantify the association between the outcome of interest (mortality and/or hospital admission) and the exposures (air-pollution and/or weather events).
Ethical approval
Not applicable for this scoping literature review as it only includes descriptive narrative analysis of 112 published articles.
A total of 112 studies ( S2 Table ) were included in the final narrative review from which 70 involved the mortality outcome, 30 the hospital admission outcome, and 12 studies included both health outcomes ( Table 1 ). Most of the studies used the time-series study design (n = 74, 66%) with Poisson models for data analysis, while minority of the reviewed studies employed the case-crossover design (n = 19, 17%) with conditional logistic regression for data analysis, and the cohort design (n = 18, 16%) with Cox hazard regression for data analysis ( Table 1 ).
https://doi.org/10.1371/journal.pone.0241415.t001
Most of the studies examined all-cause, cardiovascular and respiratory disease mortality and hospital admission outcomes while some studies tried to focus more directly on certain types of specific diseases such as psychiatric disorders including mania and depression, pulmonary embolism, myocardial infarction, stroke, ischemic heart disease, arrhythmias, atrial fibrillation, heart failure, cerebrovascular disease, chronic obstructive pulmonary disease (COPD), lung cancer, and diabetes ( Table 1 ).
Table 1 shows the descriptive statistics of the included articles. S2 Table summarise the characteristics of the included studies in more details by the type of investigated health outcome. S3 Table demonstrate the included article’s reported associations in terms of coefficients with 95% confidence intervals between air-pollution and/or weather exposure and mortality and/or hospital admission outcomes.
The effect of air-pollution on mortality and hospital admission
In this review, six air pollutants (PM2.5, PM10, O3, CO, SO2, and NO2/NOx) were identified as causes of increased rates of mortality and hospital admissions. Each pollutant affects a range of diseases, most commonly, cardiovascular, respiratory, and cerebrovascular diseases. Some of the health effects can be immediate while others might appear after several days of initial exposure ( Fig 2 ).
https://doi.org/10.1371/journal.pone.0241415.g002
The effect of particulate matter pollutants on mortality and hospital admission.
Particulate matter is a heterogeneous mixtures of liquid droplets and solid particles suspended in the air that can result either from natural resources (windblown Saharan and non-Saharan dust, volcano ashes, forest fires, pollen, etc…) or from man-made activities including industrial processes, transportation vehicle smoke, burning of fossil fuels, extensive energy usage, combustion processes, and grinding and mining industries [ 28 ]. Due to its size, mass composition, and chemical components, particulate matter with larger diameter (PM10) will be deposited in nasal cavities and upper airways while particulate matter with smaller diameter (PM2.5) may penetrate more deeply the respiratory system reaching the alveoli and blood stream, carrying with them various toxic substances [ 29 ]. This in turn will cause health problems in humans such as asthma, irregular heartbeat, nonfatal heart attacks, decreased lung function, coughing and difficulty breathing symptoms [ 30 ].
Our review showed that PM10 air-pollution is positively associated with a range of cardiovascular and respiratory diseases mortality and hospital admission outcomes ( Fig 3A and S3 Table ). Fischer et al. (2015) showed an elevated hazard of 1.06 (95% CI = 1.04 to 1.08) for cardiovascular disease mortality for every 10 μg/m3 increase in PM10 pollution in the Netherlands [ 31 ]. Likewise, PM10 pollution acted as a risk factor for respiratory diseases mortality (HR = 1.11, 95%CI = 1.08 to 1.15; RR = 1.056, 95%CI = 1.043 to 1.069) [ 21 , 32 ] and hospital admission (%increase = 0.69, 95% CI = 0.20 to 1.19) [ 20 ].
https://doi.org/10.1371/journal.pone.0241415.g003
Air-pollution with PM2.5 exhibited a similar effect on human health as that of PM10 ( Fig 3B and S3 Table ). Nevertheless, PM2.5 was shown to have a greater risk on human health as compared to PM10 due to its smaller diameter size allowing more deep penetration into the respiratory system [ 33 ]. In France, Sanyal et al. (2018) showed an increased risk of 1.11 and 1.02 for all-cause hospital admission and moratality respectively per 10 μg/m3 increase in PM2.5 pollutant [ 32 ].
The effect of ozone pollution on mortality and hospital admission.
Contrary to particulate matter pollution, the effect of ozone on mortality and hospital admission did not show a consistent effect. In some studies, ozone acted as a protective factor agianst mortality and hospital admission, while in other studies it showed increased risk or no association with mortality and hospital admissions ( Fig 3C and S3 Table ). This is related to the fact that ozone is a highly reactive pollutant and its formation is related to the presence of sunlight [ 25 ]. In a cohort study conducted by Carey et al. (2013) in England, ozone acted as a protective factor agianst all-cause mortality (HR = 0.96, 95%CI = 0.93 to 0.98), cardiovascular mortality (HR = 0.96, 95%CI = 0.94 to 0.98), respiratory mortality (HR = 0.93, 95%CI = 0.90 to 0.96), and lung cancer mortality (HR = 0.94, 95%CI = 0.90 to 0.98) [ 21 ]. However, ozone acted as a risk factor in some of the reviewed studies leading up to 2% increase in all-cause mortality per interquartile range increase of ozone concentration [ 34 – 37 ].
The effect of nitrogen oxides pollution on mortality and hospital admission.
Similar to other air pollutants, this review showed that exposure to nitrogen dioxide and nitrogen oxides pollution can cause many types of diseases resulting in increased risk for all-cause mortality and hospital admission [ 25 , 32 , 38 , 39 ] ( Fig 3D and S3 Table ). A study conducted in Belgium showed a 3.5% increase in cardiovascular hospital admission as well as 4.5% and 4.9% increase in ischemic stroke and haemorrhagic stroke hospital admissions respectively for each 10 μg/m3 increase in NO2 [ 40 ].
The effect of sulphur dioxide pollution on mortality and hospital admission.
Sulphur dioxide air-pollution is mainly caused from industrial processes and power plants that involve burning of fossil fuel. Exposure to SO2 pollution can cause mild health effects including eyes, nose, and throat irritations as well as severe health effects such as bronchial spasms and deaths due to respiratory insufficiency [ 41 ].
The effect of sulphur dioxide (SO2) on mortality and hospital admission was investigated in only 12 out of the 112 reviewed studies. Exposure to SO2 air-pollution was found to increase the risk for all-cause, cardiovascular, and respiratory mortality [ 21 , 39 , 42 ] ( Fig 3E and S3 Table ).
The effect of carbon monoxide pollution on mortality and hospital admission.
Carbon monoxide results from incomplete combustion of fossil fuels. Carbon monoxide is dangerous for human beings since it possess the ability to bind to haemoglobin resulting in reduction of the red blood cells to carry oxygen to cells [ 41 ].
Only 10 out of the 112 reviewed studies investigated the association of carbon monoxide (CO) with mortality and hospital admission. The majority of these studies showed that carbon monoxide exposure can cause a number of cardiovascular and respiratory health problems ( Fig 3F and S3 Table ). Exposure to carbon monoxide pollution resulted in increased odds for pulmonary embolism hospital admission [ 43 ]. Additionally, Renzi et al. (2017) showed that all-cause mortality increases by 0.12% for every 1 mg/m3 increase in CO [ 39 ]. On the contrary, carbon monoxide acted as a protective factor against chest disease hospital admission among patients with sickle cell anaemia in one of the reviewed studies [ 44 ]. This association was explained by the fact that carbon monoxide can bind to haemoglobin which enhances the affinity of other binding sites for oxygen in addition to reducing vasoconstriction and inflammation; suggesting a beneficial effect rather than risk factor for patients with sickle cell disease [ 44 ].
The effect of air temperature on mortality and hospital admission
Exposure to hot or cold temperature beyond region-specific thresholds exhibits a range of direct and indirect effects on human health. The direct effects include hyperthermia or heat stress during hot temperature exposures and hypothermia and ischemic stroke during cold temperature exposures [ 45 ]. Besides the direct effects, small fluctuations in temperature across time can result in indirect effects on the respiratory and cardiovascular systems of the body [ 45 ].
Most of the reviewed articles that studied the effect of weather exposure on mortality and hospital admission focused on air temperature exposure with lags ranging from 0 days up to 5 weeks for cold temperatures and from 0 days up to 25 days for hot temperatures. The reviewed studies examined the effect of cold temperature, hot temperature, and air temperature increase on a range of diseases, most commonly, cardiovascular, respiratory, and psychiatric disorders. Table 2 below shows the definitions of “cold temperature”, “hot temperature”, and “air temperature increase” classifications derived from the reviewed studies.
https://doi.org/10.1371/journal.pone.0241415.t002
Cold temperature acted as a risk factor for several types of mortality and hospital admission outcomes ( Fig 4A and S3 Table ). Nevertheless, cold temperature was a protective factor only in one of the reviwed studies for all-cause mortality at lag 0 (RR = 0.99, 95%CI = 0.985 to 0.995); yet cold temperature acted as a risk factor for all-cause mortality in the same study at lag of 14 days with a relative risk of 1.003 emphasizing the delayed effect of cold temperature on mortality [ 46 ].
https://doi.org/10.1371/journal.pone.0241415.g004
Similar to cold temperature, hot temperature also acted as a risk factor in most of the reviewed studies for a number of mortality and hospital admission outcomes ( Fig 4B and S3 Table ). On the other hand, hot temperatures were associated with reductions in hospital admission rates for ischemic heart disease (RR = 0.74, 95%CI = 0.55 to 0.99) in a study conducted by Bijelovic et al. (2017) and for all-cause hospital admissions (RR = 0.961, 95% CI = 0.956 to 0.967) and cardiovascular hospital admissions (RR = 0.975, 95% CI = 0.957 to 0.993) in a study conducted by Monteiro et al. (2013) [ 47 , 48 ].
Some studies examined the effect of increasing temperature across the whole year on mortality and hospital admission. More than half of these studies showed a significant positive association between the increasing temperature and the mortality and hospital admission outcomes ( Fig 4C and S3 Table ).
The effect of other weather exposures on mortality and hospital admission
Similar to the temperature, weather exposures that include humidity, rainfall, sunshine, snowcover, air pressure, daylight, wind speed and wind direction with lags ranging from 0 up to 7 days were found to affect a range of diseases, most commonly, cardiovascular, respiratory, and psychiatric disorders ( S3 Table ).
Weather variables that showed significant positive assciations with hospital admission included: a rainfall effect on psychiatric hospital admission [ 49 ], sunshine and daylight effects on hospital trauma [ 50 ] and psychaitric admissions [ 51 ], wind speed effects on chest disease hospital admission [ 44 ], and air pressure effects on mania and depression hospital admission [ 49 ].
It is worth mentioning that sunshine showed inconsistency in its effect on psychaitric hospital admission, acting as a risk factor in a Danish study [ 52 ] while acting as a protective factor in a study conducted in Ireland [ 49 ].
The adjustments and effect modifications for the association of air-pollution and weather exposure with mortality and hospital admission
Most of the reviewed studies stratified and adjusted their analysis by age and gender [ 25 , 40 , 51 , 53 – 61 ]. Socio-economic deprivation, education attainment, income level, marital status, and occupational class were considered as confounders or effect modifiers in some of the reviewed studies [ 25 , 58 , 62 – 66 ]. However, only one study considered ethnicity to act as an effect modifier in the association between all-cause mortality and “summer smog” days defined as having maximum temperature of 25°C and PM10 pollutant oncentration of 50 μg/m3 [ 62 ]. And only two studies investigating the effect of air-pollution on all-cause and cardiovascular mortality in England adjusted for ethnicity in their multivariate regresison models [ 67 , 68 ].
Some of the studies that examined the effect of air-pollution on mortality and hospital admission accounted for air temperature effect in their analysis [ 35 , 40 , 46 ]. Likewise, some of the reviewed articles that studied the association of weather exposure to mortality and hospital admission considered the effect of air-pollution in their analysis [ 34 , 65 , 69 – 72 ].
Other variables considered to affect the relationship of air-pollution and/or weather exposure with mortality and/or hospital admission included: weekend and holiday effect, population decrease during the summer, influenza epidemics, season, day of the week, and tobacco smoke [ 25 , 40 , 46 , 54 , 56 , 73 – 79 ].
In this scoping review of 112 articles, we aimed to examine the effect of (1) air pollution, (2) temperature, and (3) other weather exposures on mortality and hospital admission outcomes.
The first part of the review showed that air-pollution acted consistently as a risk factor for all-cause, cardiovascular, respiratory, cerebrovascular and cancer mortality and hospital admission in the EU and UK which is in line with the findings of studies conducted in other regions of the world [ 80 – 84 ]. For instance, elevated risks of cardiovascular and respiratory diseases mortality were reported in Istanbul-Turkey for every 10 μg/m3 increase in PM10, SO2 and NO2 pollutants [ 85 ]. An exception was ozone (O3) air-pollution which showed inconsistent association with mortality and hospital admission. Two explanations were offered in the literature for the negative association between health outcomes and ozone pollution. The first explanation is related to the fact that ozone is a highly seasonal pollutant since its formation is catalysed by sunlight rendering higher ozone concentrations in the summer as compared to winter season. Thus, ozone effect on health outcomes should be analysed by accounting for the season effect [ 21 ]. In the continental United States, a 49% higher risk in all-cause mortality was shown for every 10 ppb increase in ozone during the warm-season [ 86 ]. The second explanation is related to the high reactivity of ozone leading to the formation of other pollutants such as NO2 and particulate matter. Therefore, ozone is negatively correlated with other air pollutants and its effect on health outcomes should be analysed as a combined effect of O3 and NO2 (known as Ox effect) [ 25 ].
Additionally, our scoping review showed that the effect of particulate matter (PM10 and PM2.5) pollution on mortality and hospital admission is more studied in the literature as compared to the other air pollutants. This could be related to the more pronounced effects of particulate matter exposure on health which is corroborated by many studies across the world [ 81 , 87 ]. Despite the fact that PM10 particles are deposited in the nasal cavities and upper airways, PM2.5 may penetrate deep into the lung tissues (reaching the alveoli and bloodstream) and irritate the respiratory airways causing various respiratory and cardiovascular problems [ 29 , 30 , 88 ].
Similar to air pollution, the second part of this review showed that hot and cold temperature exposures beyond region-specific thresholds are risk factors for a wide range of respiratory, cardiovascular (including: ischemic heart disease, myocardial infarction, pulmonary embolism, stroke, heart failure, and COPD), and psychiatric (including: mania and depression) illness in the EU and UK. These findings are corroborated by a wide body of literature from across the world [ 89 – 97 ]. In India, cold temperatures below 13.8°C were associated with increased risk of 6.3% for all-cause mortality, 27.2% for stroke mortality, 9.7% for ischemic heart disease mortality, and 6.5% for respiratory diseases mortality [ 92 ]. In Istanbul-Turkey, 23 days of exposure to hot temperature above 22.8°C was associated with a total of 419 excess deaths [ 90 ]. In Korea, hot temperature days of 25°C compared to 15°C were significantly associated with a 4.5% increase in cardiovascular hospitalizations [ 98 ].
It is worth to point out that the effect of cold temperature on health is more delayed (up to 5 weeks) in comparison to the more immediate effects of hot temperature (up to 25 days). Similar study in Northeast-Asia showed a delayed risk of cold temperature on mortality after 5 to 11 days, yet a more immediate effect of hot temperature on mortality after 1 to 3 days in each of Taiwan, Korea, and Japan countries [ 91 ].
Although exposure to hot or cold temperature can affect the health negatively, our scoping review showed that in few studies, the increase in temperature reduced the risk of hospital admissions for some types of cardiovascular diseases; mainly for pulmonary embolism, angina pectoris, chest, and ischemic heart diseases. This could be explained by the fact that hot temperature can cause immediate increase in cardiovascular mortality rates; whereby many cases might pass directly to the death state without passing through the hospital admission state resulting in lower hospital admission rates [ 47 ].
The third part of this scoping review presented the studies that examined the effects of other weather exposures such as relative humidity, barometric pressure, rainfall, and wind speed on mortality and hospital admission outcomes. These weather exposures were found to affect significantly only hospital admission. No significant effect was noted with respect to the mortality outcome. The weather exposures acted as a risk factor for psychiatric disorders (including depression and Mania), chest disease, and trauma hospital admissions. This was corroborated by evidence from countries outside the EU as well [ 99 – 101 ]. Yet in some of the reviewed studies, weather exposures acted as a protective factor for some types of psychiatric and cardiovascular disorders. The significant negative association between ischemic heart disease hospital admission and humidity in one of the reviewed studies was explained by the fact that people in general and the elderly specifically reduce their activities during high humidity and temperature periods. This is mainly due to the lack of the body’s ability to perspire, which in turn reduces their risk of cardiovascular complications [ 48 ]. As for the protective effect of some weather exposures on psychiatric hospital admissions, similar findings were presented in Iran; with a negative association between barometric pressure and schizophrenia hospital admissions and rainy days and bipolar hospital admissions [ 101 ].
In addition to the association of air pollution and weather exposure with mortality and hospital admission outcomes, our review aimed to present the individual, socio-economic, and environmental factors that play an important role in modifying the latter association. The effect modifiers identified in this scoping review included: pre-existing health conditions, age, gender, educational attainment, wealth or income or socio-economic deprivation, occupation, marital status, tobacco smoking, season, day of the week, holidays, and influenza epidemics.
Individuals with pre-existing chronic health conditions face increased susceptibility toward air-pollution and weather exposure related mortality and hospital admission [ 52 , 54 , 78 , 102 ].
Older people are more vulnerable to the health effects associated with air-pollution, hot or cold temperatures, and other weather variables [ 54 , 56 , 103 – 105 ]. This is due to the physiological degeneration of the human body with increasing age. Aging affects the normal function of the body organs resulting in many chronic cardiovascular, urinary, and respiratory health conditions. This reduces the ability of older people to adapt to increased concentrations of air pollutants and changing weather conditions [ 103 , 105 , 106 ]. Moreover, old age people have lower immunity and antioxidant defence as compared to young people placing them at a higher risk [ 107 ]. Many older people also have reduced mobility and mental abilities which delay their access to healthcare leading to severe health complications and death [ 108 ].
As for gender, our review revealed inconsistency regarding its modification effect on the association between air-pollution and weather exposure and mortality and hospital admission health outcomes. Nevertheless, most of the reviewed studies have found that females have higher risks of mortality and/or hospital admission after exposure to air-pollution and/or weather fluctuations beyond region-specific thresholds including hot and cold temperatures [ 9 , 47 , 57 , 58 , 65 , 78 , 109 – 112 ]. Whereas some studies found higher risks of mortality and/or hospital admissions among males in relation to air-pollution and/or weather exposure [ 25 , 40 , 42 , 59 , 70 , 113 , 114 ]. One explanation for this might be due to the physiological differences between males and females. Females have smaller lung size, yet higher airways reactivity making them more susceptible to air-pollution health effects as compared to males [ 42 , 115 ]. Likewise, higher pulse rates and smaller heart size relative to the human body in females as compared to males render females more vulnerable to the health effects of air-pollution and hot or cold temperature exposures [ 115 ]. Moreover, females exhibit more fluctuations in hormone levels due to pregnancy, menstrual cycle and menopause periods which may place them at a higher health risk upon exposure to air-pollution and weather variations [ 115 ]. The different lifestyle, socio-economic position, and occupation type between males and females may also lead to different levels and duration of air-pollution and weather exposure [ 62 , 109 , 116 – 118 ]. However, it is worth mentioning that the effect modification of gender in the association of air-pollution and weather exposure with mortality and hospital admission outcomes is believed to be confounded by age since in many of the reviewed studies, higher risks were found among old aged females (age>65 years old) [ 47 , 57 , 61 , 78 , 112 ] and old aged males (age >70 years old) [ 114 ]. This confounding effect could be reduced either by assessing the combined effect modification of age and gender through an interaction term or by stratifying the analysis according to both the age groups and gender.
Wealth and socio-economic deprivation were also considered by some of the reviewed studies as an effect modifier in the relationship of air-pollution and weather with mortality and hospital admission. In general, the absence of wealth and presence of socio-economic deprivation increase the risk of exposure to air-pollution and weather variations resulting in elevated mortality and hospital admission rates in Europe [ 62 , 66 , 76 ] and in other parts of the world including New Zealand [ 22 ], United States of America [ 119 ], and Chile [ 120 ].
Educational attainment was also considered by some of the reviewed studies as an effect modifier, with higher risks detected among individuals with lower educational attainment [ 25 , 63 , 64 , 121 , 122 ]. Despite the consideration of age, gender, education, and wealth effect in the association of air-pollution and weather with mortality and hospital admissions in Europe, our scoping review revealed the lack of investigation into the role of other important socio-demographics such as ethnicity. Research has extensively shown that ethnic minorities live in more disadvantaged communities and have lower socio-economic status as well as poor housing conditions. This results in higher risk for chronic health problems associated with higher exposure on one hand and with lower access to quality healthcare on the other hand [ 22 – 24 ].
Finally, it is worth to note that most of the reviewed studies with a time-series or case-crossover design adjusted their analysis for the season effect [ 40 , 46 , 52 , 54 , 60 , 71 , 73 , 74 , 123 , 124 ]. It is well established that air-pollution, temperature, and other weather variables vary with seasons [ 125 – 127 ]. Not to mention that the emission, formation, and dispersion of air pollutants is affected by seasonal weather variations which in turn affects the individual exposure levels [ 128 ]. Outdoor activities and daily habits (eg. Window ventilation of houses) might also vary depending on the season which reflect changes in the level and duration of individual exposure to air-pollution and weather changes [ 129 ].
Despite the value of this scoping literature review, it has some limitations. First, the employed search strategy was limited to original articles published in peer reviewed journals which might have led to the omission of unpublished work or articles that were published in non-indexed journals. Nevertheless, our search strategy involved navigation through two databases which enables a good catch of major published studies addressing the effect of air-pollution and weather exposure on mortality and hospital admission. Second, limiting our inclusion criteria only to English language articles might have resulted in missing some research written in other languages. However, as most of the literature worldwide is published in the English language, we believe that no major papers have been excluded. Third, this review was limited only to quantitative research which would have led to missing out other type of important research including opinion research pieces and letters to editor as well as qualitative research studies. Opinion research pieces and letters to editor provide a critical appraisal/discussion for the findings of original studies which warrant future research development. Qualitative studies provide an overview about the effect of air-pollution or weather variations on human health from the perspective of lay people rather than relying only on objective census/statistics numbers as in quantitative research. Forth, due to resources limitations, title and abstract screening as well as data abstraction were done only by one researcher (MA). Nevertheless, a second researcher performed title and abstract screening for a random sample of 20% of the retrieved records. Given the high consensus between the two researchers, we are confident of the exact application of the inclusion and exclusion criteria. Our goal from this literature review was not to produce a numerical estimate but rather to give a narrative summary on the effect of air-pollution/weather on mortality/hospital admission. Hence, missing some studies would not be a major concern for this scoping review.
Literature gaps and implications for future research
This scoping review helped us to identify literature gaps that require further research.
First, this review revealed the extensive research carried out to determine the effect of air-pollution on human health. Yet, due to the high correlation between air pollutants and the issue of collinearity in multivariate models, most of the studies examined the effect of single pollutants on mortality and hospital admission outcomes. Nevertheless, the issue of correlation between air pollutants is highly contextual and it depends on the study settings including the season and the specific geographical area. Hence, future researchers should try to examine the effect of multi-pollutants on mortality and/or hospital admission in one model, where strong correlations between the air pollutants are absent.
Second, the majority of studies examined the direct effects of air-pollution and weather exposure on mortality and hospital admission without considering the role of certain effect modifiers. The examined effect modifiers considered mostly by the literature involve age, gender, education, socio-economic deprivation, and season. Therefore, there is a lack of evidence regarding the modifying effect of other individual factors such as previous disease conditions and ethnicity which affect the person’s health vulnerability. Indeed, future research is needed to find out the reasons behind elevated individual’s susceptibility to the detrimental effects of air-pollution and weather variations in certain groups of population.
Third, our review showed that most of the studies either investigated the effect of air-pollution or the effect of weather on mortality and hospital admission. The formation and dispersion of air pollutants depends highly on the existing atmospheric conditions such as temperature, humidity, and wind speed [ 130 ]. Therefore, future studies should consider examining the effect of both, weather conditions and air-pollution, on human health through interaction terms or adjustments in the analysis models.
Fourth, although extensive research has been performed to study the effect of particulate matter and nitrogen oxides pollution on human health, there was a lack of research with respect to other air pollutants including carbon monoxide, ozone, and sulphur dioxide. This might be due to the absence of rigorous and reliable measurements of these pollutants or due to the complexity of analysing the effect of these pollutants.
Fifth, literature is more focused on examining the effect of temperature on mortality and hospital admission, placing less emphasis on other weather exposures. Hence, future research should shift the focus toward other weather exposures such as wind speed, rainfall, humidity, snow cover, daylight, and air pressure.
Sixth, there was a lack of research examining the effect of air-pollution and weather on hospital admission. Mortality was the major outcome in most of the reviewed studies due to the ease of data access governed by less ethical considerations. Additionally, analysis is more straightforward given that it occurs only once in an individual’s life. Thus, it is recommended for future research to consider the impact of air-pollution and weather variables on hospital admission on its own and in combination with mortality through multistate modelling.
Finally, the majority of studies in this field employ the time-series design which uses aggregated mortality and hospital admission data linked to environmental exposures at the local authorities or municipalities level. Research that uses aggregated data neglect the physiological and socio-economic differences among individuals. Additionally, assigning air-pollution and weather exposure based on wide geographies overlook the small geographical exposure differences biasing the drawn estimates. Therefore, there is a need for cohort research studies that utilize individual level data linked to air-pollution and weather exposure at small geographical spatial resolution (eg. Postcodes).
In summary, our scoping review showed that air-pollution and weather exposure beyond certain thresholds lead to various impacts on human health, most commonly cardiovascular and respiratory problems, resulting in increased rates of mortality and hospital admission. Yet, further research is needed given that the effect modification of important socio-demographics such as ethnicity and the interaction between air-pollution and weather is often missed in the literature. Understanding this should give enough evidence to the policy makers to plan and act accordingly aiming to reduce the effects of air pollution and weather variations on the public health. Additionally, research should focus on projecting future health behaviour and mortality patterns in relation to air pollution and weather variations, in order to guide effective environmental and health precautionary measures planning.
Supporting information
S1 checklist. prisma checklist followed for this systematic scoping review data searching, screening, and abstraction..
https://doi.org/10.1371/journal.pone.0241415.s001
S1 Table. The search codes used in PubMed and Web of Science databases for this scoping literature review.
https://doi.org/10.1371/journal.pone.0241415.s002
S2 Table. A detailed summary of the characteristics of the 112 studies included in this scoping review by the type of investigated health outcome.
https://doi.org/10.1371/journal.pone.0241415.s003
S3 Table. A detailed summary of the reported associations between air pollution and/or weather exposures and mortality and/or hospital admission outcomes in the 112 reviewed studies in terms of coefficients and 95% confidence intervals.
https://doi.org/10.1371/journal.pone.0241415.s004
Acknowledgments
The authors would like to thank the University of St Andrews Library services for helping in developing the search codes used in this scoping literature review.
- View Article
- PubMed/NCBI
- Google Scholar
- 3. World-Bank. Cities and Climate Change: An Urgent Agenda. Washington DC: The World Bank; 2010.
- 5. WHO. Ambient (outdoor) air pollution: World health organization (WHO); 2018 [Available from: https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health
- 27. European-Commission. EU action against climate change: Leading global action to 2020 and beyond Luxembourg: Office for Official Publications of the European Communities; 2009. Contract No.: KH-78-09-725-EN-C.
- 41. Samet J, Jaakkola J. The epidemiologic approach In Air pollution and health (Holgate ST, Samet JM, Koren HS and Maynard RL, Eds.). Academic Press, London; 1999.
- Research article
- Open access
- Published: 28 November 2017
A systematic review of data mining and machine learning for air pollution epidemiology
- Colin Bellinger ORCID: orcid.org/0000-0002-3567-7834 1 ,
- Mohomed Shazan Mohomed Jabbar 1 ,
- Osmar Zaïane 1 &
- Alvaro Osornio-Vargas 2
BMC Public Health volume 17 , Article number: 907 ( 2017 ) Cite this article
27k Accesses
153 Citations
12 Altmetric
Metrics details
Data measuring airborne pollutants, public health and environmental factors are increasingly being stored and merged. These big datasets offer great potential, but also challenge traditional epidemiological methods. This has motivated the exploration of alternative methods to make predictions, find patterns and extract information. To this end, data mining and machine learning algorithms are increasingly being applied to air pollution epidemiology.
We conducted a systematic literature review on the application of data mining and machine learning methods in air pollution epidemiology. We carried out our search process in PubMed, the MEDLINE database and Google Scholar. Research articles applying data mining and machine learning methods to air pollution epidemiology were queried and reviewed.
Our search queries resulted in 400 research articles. Our fine-grained analysis employed our inclusion/exclusion criteria to reduce the results to 47 articles, which we separate into three primary areas of interest: 1) source apportionment; 2) forecasting/prediction of air pollution/quality or exposure; and 3) generating hypotheses. Early applications had a preference for artificial neural networks. In more recent work, decision trees, support vector machines, k-means clustering and the APRIORI algorithm have been widely applied. Our survey shows that the majority of the research has been conducted in Europe, China and the USA, and that data mining is becoming an increasingly common tool in environmental health. For potential new directions, we have identified that deep learning and geo-spacial pattern mining are two burgeoning areas of data mining that have good potential for future applications in air pollution epidemiology.
Conclusions
We carried out a systematic review identifying the current trends, challenges and new directions to explore in the application of data mining methods to air pollution epidemiology. This work shows that data mining is increasingly being applied in air pollution epidemiology.
The potential to support air pollution epidemiology continues to grow with advancements in data mining related to temporal and geo-spacial mining, and deep learning. This is further supported by new sensors and storage mediums that enable larger, better quality data. This suggests that many more fruitful applications can be expected in the future.
Peer Review reports
The decreasing costs of remote sensors for measuring airborne agents, along with the increasing availability of environmental and clinical data, has led to an explosion in the number of pollution datasets available for analysis. These datasets often have a very large number of samples and tend to have a significant number of variables with mixed degrees of dependencies. These big datasets come with complexity that renders it difficult to rely on traditional epidemiological or environmental health models to analyze them. As a result, new methods of analysis are required in order to advance our understanding of the data. Data mining and machine learning methods from computing science present a wide array of scalable and reliable methods that have performed well on similar problems in other domains. This has inspired a burgeoning field of research within Environmental Health aimed at the adoption of data mining methods to analyze modern, big datasets in air pollution epidemiology inefficient and effective ways.
Data mining is the computational process that is often applied to analyze large datasets, discover patterns, extract actionable knowledge and predict outcomes of future or unknown events. Methods used in this process come from a combination of computational disciplines including Artificial Intelligence, Statistics, Mathematics, Machine Learning, and Database Systems. Apart from the core methods used to carry out the analysis, the process of data mining can involve various preprocessing steps prior to executing the mining algorithm. In addition, a post-processing stage is typically employed to visualize the results of the analysis (i.e. recognized patterns or retrieved information) in an intuitive and easy-to-communicate manner. In this review, we limit our scope to focus on core data analysis techniques as they have been applied to the field of air pollution epidemiology and reported within the air pollution epidemiology literature.
In a broad sense, there are two major paradigms of algorithms: prediction and knowledge discovery. Within these, there are four sub-categories: 1) Classification and regression, 2) Clustering, 3) Association Rule Mining, and 4) Outlier/Anomaly Detection. In addition, there are some relatively new and exciting areas of data analysis, such as spatial data mining and graph data mining, that have been made possible via the building blocks of data mining methods.
According to the best of our knowledge, there are no studies that investigate the depth and breadth of the application of data mining methods within air pollution epidemiology. With this in mind, we perform an investigation to identify which data mining methods have been applied, and to which areas of air pollution epidemiology they have been applied to. Our goal is to point domain researchers to preexisting data mining applications in their areas, and related areas, as well as advance their understanding of the potential of data mining and inspire them to explore further research avenues.
Methodology and paradigms of data mining algorithms
Data mining algorithms are particularly beneficial on complex datasets with a large number of variables and samples. With respect to knowledge discovery, they add insight into high-dimensional problems where traditional statistical methods often fail. Similarly, machine learning algorithm can induce accurate predictor functions from complex, high-dimensional datasets where statistical and mathematical methods, such as regression, can be prone to inaccuracies and be difficult to apply due to their underlying assumptions.
Considerations for applying data mining
In order to implement a successful data mining solution, the user must analyze and formalize their objective. The problem objective guides the user to the appropriate paradigm of learning algorithm. If the objective is to identify hidden groups in data or identify associations between key variables in the data, the users are interested in knowledge discovery and will want to select a clustering or association mining algorithm. Alternatively, the objective might be to induce a predictive model that can classify samples as belonging to a particular category, such as poor air quality, or a real-valued outcome, such as the air quality index.
A large and growing number of algorithms belong to the prediction paradigm and the knowledge discovery paradigm. How to choose between the methods within each paradigm is a topic in its own right. To assist practitioners that are new to the application of machine learning algorithms, Domingos discusses the some of the key considerations in [ 1 ].
When making this decision, the user should consider the complexity of the problem and the amount of data available. A simple, linear classifier, for example, will be ineffective on a complex non-linear classification problem. A large volume of data will facilitate the use of advanced learning algorithms, such as deep artificial neural networks [ 2 ], however, it also forces users to consider questions related to storage, memory and training time.
In general, it is widely understood that there is no silver bullet when it comes to learning algorithms. From an application perspective, a good practice is to select a small, diverse set of algorithms from the paradigm of relevant methods, test them individually and select the one that best meets the performance objectives. Alternatively, grouping a diverse set of models to form an ensemble of predictors has been demonstrated to be an effective solution in theory and practice [ 3 ]. Within the surveyed literature, for example, [ 4 ] applied an ensemble formed of neural networks, support vector machines, Gaussian processes, decision trees and random forests.
Once a set of potential algorithms has been selected, the models that are induced by each algorithm over the available dataset must be evaluated in order to select the one model, or ensemble, that is most likely to preform the best on the prediction task in the future. This is an area of research that is presented in Error Estimation for Pattern Recognition [ 5 ] and Evaluating Learning Algorithms [ 6 ].
The paradigms of learning that have most widely been applied in air pollution epidemiology can be categorized as prediction-based or knowledge discovery methods.
Value prediction
Value prediction is a common and widely applicable area of data mining in which the objective is to take in a set of variables related to an instance drawn from an underlying sample population and predict the corresponding value. Depending on the nature of the application, the user will choose either a data mining algorithm that makes categorical predictions (a classifier) or numeric predictions (similar to regression.) Typical classification algorithms include decision trees, Bayesian classifiers, support vector machines and multilayer perceptrons. Artificial neural networks, support vector regression and regression trees are typical data mining methods for performing numeric predictions. The standard approach to select the most appropriate method for a given problem, such as a classification problem, is to perform repeated trials with multiple classifier algorithms and select the approach that performs the best on the learning problem.
More formally, prediction algorithms are typically induced through a process of supervised learning. The objective is, thus, to make predictions y about instances x of the target problem. For this, a parametrized function \(\mathcal {F}: x \rightarrow y\) is induced. The prediction problem can be one of discrete value prediction, such as classifying breast cancer, or continuous value prediction, much like regression.
In order to perform supervised learning, a dataset X of examples, such as patient information, and corresponding values (or labels) Y , are compiled and used for model induction. Each row of X is a feature vector x =( x 1 , x 2 ,..., x n ). The features x i are equivalent to the data variables in a statistical context. The label set, Y ∈ { y 1 , y 2 ,... y n }, specifies the value that each corresponding instance x i takes. In discrete prediction tasks, the class labels are typically mutually exclusive but do not necessarily have to be [ 7 ]. For continuous values prediction, the value space typically involves real numbers, \(Y \in \mathcal {R}\) , but can also apply to integers, \(Y \in \mathcal {I}\) .
Decision trees, Bayesian methods, support vector machines and artificial neural networks are the most common supervised learning algorithms. We provide a brief overview and direct the reader to [ 8 ] for a detailed description of these algorithms.
Decision trees are simple, but an often effective form of learning classifiers, regressors, and rules. The induction process applies a divide-and-conquer strategy which partitions the data space based on the feature values. Decision trees are often preferred over the more sophisticated models that we discuss below in fields such as medicine because the decisions leading to their predictions can be understood by humans. A very simple example of the interoperability comes from a hypothetical flu classifier which makes predictions { FEVER = TRUE ∧ HEADACHE = TRUE ∧ COUGH = TRUE → FLU = TRUE }.
The standard tree induction algorithms are CART, ID3 and C4.5 [ 9 – 11 ]. Decision trees are induced in a top-down manner by recursively selecting a feature that best divides the training instances according to their labels. A notion of purity known as information that is measured in units of bits is commonly used to measure purity in the determination of the best feature f i at the current level l i . Branches from level l i to level l i −1 are then created; one branch is made for each potential value of f i . The training set is partitioned based on the branches from l i to l i −1 and the process is repeated for each node in level l i −1 . The recursive process stops when the leaves only contain instances from a single class. It should be noted, however, that a form of pruning must be applied to the tree to avoid overfitting.
Artificial neural networks are a powerful form of learning algorithm with a long tradition in pattern recognition and machine learning. Their foundation comes from mathematical attempts at replicating information processing in biological systems [ 12 ]. In modern applications, however, they deviate significantly from the roots of their biological inspiration.
With modern memory and processing power, there is a great potential for complex artificial neural network architectures such as convolutional networks and recurrent network that have seen recent success in deep learning [ 2 ]. The standard architecture, however, is a feedforward network known as a multilayer perceptron. The name refers to the fact that the network is a directed graph that is typically composed of three or more layers. The nodes in the first layer are connected to the nodes in the second layer and so on. The first layer is the input layer. This is where the feature vector x enters the network. It is passed successively through the layers of the network until it reaches the final layer, the output layer. The layers between the input and the output layers are known as hidden layers. Each hidden layer is composed of a user-specified number of hidden units (the nodes in the directed graph).
For each unit i of each hidden layer l , the value of the unit \(h^{(l)}_{i}\) is calculated as the values of the units connected to \(h^{(l)}_{i}\) from the layer below as:
where i is the number of units in the previous layer, j is the specifies the unit in the current layer, ω ji is the parametrized weights connecting layer l −1 to the current layer, l , for unit j , and b l is the bias applied to the current layer.
An activation function is applied to hidden value \(\mathbf {h}^{(l)}_{j}\) . The choice of a non-linear activation, such as sigmoid , enables the model to learn a non-linear representation of the data. However, regularized linear units have recently been found to be useful in the hidden layers [ 13 ].
Multilayer perceptrons are typically trained via back-propagation with gradient descent. This involves updating the weights of the network over multiple iterations of the training set. This is a non-convex optimization process, and thus, training may get stuck in local minima. In practice, however, the models have been found to be very effective.
Support vector machines (SVM) are a powerful method for solving classification and regression problems based on the calculation of the maximum margin hyperplane [ 14 , 15 ]. For non-linear SVM, the data is mapped to a higher dimensional space via a user-specified kernel, such as a polynomial kernel or a radial basis function. The maximal margin hyperplane is implicitly found in this higher dimensional space, the result of which can be a non-linear decision boundary in the original space. A key property of SVM is that model induction is a convex optimization problem. As a result, any local minima is also a global minima.
The maximum margin classifier is of the form y ( x )= w T θ ( x )+ b , where x is a query instance, w is the maximum margin hyperplane, θ is a kernel function, and b is an offset.
The maximum margin hyperplane is solved via:
where x n and y n are the training instances and labels. Directly solving this optimization problem is very complex, however, it can be converted to a simpler, but equivalent problem using the Lagrangian dual which is solvable via quadratic programming. Finally, for kernels satisfying the property k ( x i , x j )= θ ( x i )· θ ( x j ) the kernel trick is used to avoid performing the computations in the kernel-space.
Knowledge discovery
Clustering algorithms are a form of knowledge discovery performed via unsupervised learning. They group the instances of a dataset X into k clusters based on an algorithm specific notion of similarity. The process is termed unsupervised because the algorithms do not use a label set for learning. As a result, the process is one of knowledge discovery that infers the groupings from the data.
Similar to classification and regression, a wide variety of clustering algorithms have been developed. Selecting the right algorithm is domain dependent. Nonetheless, the k-means algorithm remains one of the most prominent clustering techniques. It is often preferred for its simplicity and theoretical foundation.
K-means employs an iterative process of updating the cluster centres that repeats until convergence. The k in k-means refers to the user-specified number of clusters. Initially, the k centres are set at random. Subsequently, each instance in X is assigned to the cluster of its nearest centre. The k centres are then updated to be at the centre of their assigned group. Convergence occurs when the centres stop moving.
In spite of its popularity, k-means has some well-known weaknesses, such as susceptibility to outliers. The Density-based clustering algorithm DBSCAN is an alternative method designed to account for noisy instances and outliers. In addition, one can manufacture scenarios in which k-means will fail to define good clusters under certain conditions.
Hierarchical clustering is a form of distance-based clustering that creates hierarchies of clusters. The clusters are either built agglomeratively or divisively. The former commences by assuming each instance of X belongs to its own cluster and builds up the hierarchy by successively merging clusters. Alternatively, the divisive approach starts with all instances in one big cluster and recursively splits the clusters into smaller clusters down the tree. This form of clustering is very effective for visualizing the groupings and different levels of granularity.
Association rules are similar to the rules extracted from decision trees and produced by rule-based classifiers. The key difference is that in association rule mining, the notion of class categories is not utilized in the rule induction process.
In association rule mining, a dataset X is given in which the rows are instances and the columns are the feature, F ∈ { f 1 , f 2 ,..., f n }, that quantify the instances. In medical domains, the features could be has _ cough ∈ { yes , no }, fever _ level ∈ { none, low, medium, high }, has _ headache ∈ { yes, no }, etc .
Through association rule mining we aim to generate a set of interesting rules from X of the form A → B , where A ⊂ F and B ⊆ F . In contrast, rule-based classifiers learn rules of the form A → B , where A ⊂ F and B ∈ Y ; here, Y is the set of possible class labels.
Given the definition of an association rule, any unique combination of the features, F , can appear on the left side and the right side of the implication. As a result, an enormous number of rules can be generated. Many of these, perhaps the majority, would be uninteresting according to any reasonable assessment. Thus, the rules must be filtered or pruned, as to only keep the valuable rules. Individually assessing each rule in a brute-force manner is prohibitive, and thus, more efficient methods of rule induction have been developed.
The APRIORI algorithm is the most common technique of association mining [ 16 ]. The key to their strategy is the employment of an iterative process that builds up frequent item sets and association rules from their simplest form (one-item sets) to the complex (two-item sets, three-item sets,..., n-item sets). An example of a one-item set and a two-item set from our medical domain is has _ cough = yes , and has _ cough = yes ∧ fever _ level = none . The items are deemed to be frequent if they have more than a user-specified number of necessary occurrences s in the dataset.
The algorithm gains its efficiency from the realization that if a one-item set, such as has _ cough = yes , is not frequent in the dataset, then no two-item set including the one-item set, such as has _ cough = yes ∧ fever _ level = none , can be frequent. Therefore, the algorithm can ignore all higher-order rules involving has _ cough = yes . In general, the algorithm commences by finding all frequent one-itemsets and then finds candidate two-items sets from the frequent one-item sets. The two-itemsets that are frequent are kept, and the process repeats until some point, k , is reached where no k -itemsets are frequent.
In the last stage, all of the frequent itemsets are used to form association rules. The frequent item set A 1 ∧ A 2 ∧ A 3 , for example, generates A 1 → A 2 ∧ A 3 , A 1 ∧ A 2 → A 3 , etc . A similar bottom-up methodology is applied here to efficiently generate rules that meet the minimum frequency requirement.
We have undertaken this survey in a systematic manner guided by the work of Kitchenham in [ 17 ] and the PRISMA standards [ 18 ]. Accordingly, the strategy for conducting this survey is detailed in the following sub-sections. In addition, we have taken motivation for the organization of this survey from a related survey on dengue disease surveillance [ 19 ].
Research questions
The primary research questions considered in this survey are:
R1 To what degree has data mining been applied in air pollution epidemiology?
R2 Are there any hotbeds of this research area?
R3 To which sub-fields of air pollution epidemiology has data mining been applied?
R4 Which data mining methods have been applied?
R5 What are the limitations of the current work?
R6 What potentially fruitful directions remain unexplored?
With respect to R1, we searched the relevant epidemiological literature for research employing data mining techniques. We did not place any bounds on the dates, however, it is clear that the active period is relatively small. Moreover, there is an upward trend in the frequency as the benefits of data mining become more widely known, and tools that lower the barriers to use are made available.
Following from R1, R2 considered if the existing research is uniformly spread around the countries and institutions of the world, or if particular countries and institutions have a more keen focus on researching this area.
To address R3, we filtered through the identified articles to find any reasonable sub-categorization of the epidemiological work in terms of the application areas. This process revealed three categories of epidemiological studies of air pollution in the literature involving data mining.
In R4, we looked to see which paradigms, and which algorithms, have been applied in the air pollution epidemiology literature. From this vantage point, we found that four classes of methods have been applied.
For research question R5, we considered if, given the objectives, the data and/or the mining algorithms applied had any limitations. Given our backgrounds in data mining, we were particularly focused on the data used, algorithms applied and the processes by which the methods were evaluated.
Finally, in R6 we considered the reasonable next steps. Once again, our consideration here took a data mining perspective. To this end, we were interested in identifying new ways of using the existing data and cutting edge data mining algorithms that should be tested within this research domain.
Search process
We performed a temporally unbounded search for articles listed in the PubMed database 1 , the Public Library of Science (PLOS) 2 and Google Scholar 3 . This includes articles published up to the time of writing in October 2017.
The articles reported herein result from a three-part search procedure. This involved: a ) a query-based search to produce a long list of potential articles designed and conducted by CB and MSMJ, b ) a fine-grained manual evaluation of the long-listed articles by one author performed by CB and MSMJ, and c ) identified articles were reviewed by the remaining authors (AOV and OZ). The queries applied to the database and with the number of articles returned are reported in Table 1 .
We excluded articles that did not go through a peer review process in recognized biomedical publication, and articles that did not apply one or more data mining algorithms. Many environmental health articles, for example, mention, and/or discuss, the potential for data mining but did not applying data mining methods. Articles that discuss data mining in the future work were returned by our queries, but are not appropriate for inclusion in our survey.
Data extraction and synthesis
The following information was extracted from each of the selected articles:
The source (journal or conference) and full reference.
A summary of the objective of the study.
The air pollutants of interest in the study.
The data mining method applied to achieve the objective.
A summary of the findings of the study.
This information was extracted by CB and MSMJ and validated by AOV and OZ. Any disagreements were handled via discussion and common consensus. After the raw details of the articles were tabulated, data synthesis was performed. In addition, AOV extracted information about each article related to the biomedical objectives.
Data synthesis involved analyzing the objectives, data mining methods, and the target pollutants in order to identify categories to effectively group the various studies. This exercise was performed by CB and reviewed by the remaining authors. Our goal in the categorization was to identify a hierarchy of categories that provided a sketch of the research landscape. In addition, the purpose was to facilitate quick and easy locating of the studies that are related to the reader’s area of interest. The identified categories are listed below:
Physical Area
Outdoor (Rural, Urban and General 4 )
Forecasting and Prediction
Source Apportionment
Hypothesis Generation
Data Mining Method
Classification
Association Mining
Aspects of data mining in air pollution epidemiology
Environmental setting: overview.
In this section we discuss the target areas of interest (the environmental setting). We have separated these into indoor, outdoor and general. Indoor refers the studies focused on indoor air pollution, such as air pollutants measured within the home or workplace. Outdoor refers to studies interested in outdoor air pollution, such as air pollution measured at a specific intersection or the dispersion of pollutants across an area of interest. It can be further separated into urban, metropolitan and rural. Given that the current breadth of research is still relatively sparse, we focus on the top level of abstraction in this article. We note, however, that a large portion of the research in the outdoor category has been applied to urban and/or metropolitan settings. This is, perhaps, not surprising given that the high population density in metropolitan areas can lead to high impact research. Nonetheless, it suggests rural environments as a potential direction for future work.
The general category covers research that applies data mining methods to study the health impacts of combinations of chemicals common in air pollution. These studies were typically conducted in laboratory settings rather than in the field (or relying on data collected from the field). Table 2 includes a categorized list of articles in relation to their environmental settings.
Categorized study objectives: overview
We grouped the selected articles into the following general study objectives: forecasting and prediction, source apportionment and hypothesis generation. A large percentage of the articles identified in our survey dealt with forecasting or predicting pollution levels based on various climatic and/or pollutant values. These studies considered: a ) forecasting future pollution levels at a specific location given some specific data for that location, b ) forecasting current pollution levels at a specific site given some regional data, and c ) forecasting the geo-spatial distribution of air quality or the spread of pollutants.
Closely related are the studies that were designed to predict increases in sickness or hospitalization from climatic and pollution measurements or to classify sickness in individuals given an air quality or pollution assessment.
Studies classified into the source apportionment category aimed to trace a given decrease in air quality or increase in a given pollutant back to its emission source given a set of pollutant and climatic variables.
Finally, a large number of articles performed hypothesis generation. These studies take in the wide variety of data available about the evolution of air pollution at a specific location, its spread across a region or the globe, health indicator variables, etc ., and use data mining algorithms to identify hidden associations between the variables. These associations are used to test existing assumptions and generate new ones. Exemplary associations might indicate that a certain chemical combination X,Y,Z is associated with increased volume in the emergency department at a hospital of interest, or that climatic conditions W,R combined with heavy seaport traffic, lead to a decrease in the air quality index. These associations can serve to motivate focused trials to study the discovered relationship in depth.
Table 3 includes the articles in a list sorted according to the objectives of the research. It is worth noting that a given article may have more than one objective, and thus, may appear multiple times in the table.
Summary statistics
Prisma results.
The summary statistics recording the numbers of articles returned from our search process, excluded, and included are presented in the PRISMA flow chart in Fig. 1 . Our initial search returned 400 articles. In addition to these, one article ([ 20 ]) was suggested during the review process. After the initial screening and eligibility assessment, 47 articles were included in this survey.
PRISMA flow diagram. Overview of the PRISMA results from our search process
Regional and temporal overview
We have found that eighteen of the studies were from Europe and the UK, sixteen were from the USA, ten were from China, and four were from other Asian countries. The detailed breakdown of this is provided in Fig. 2 . The papers were published between 2000 and October 20, 2017. Figure 3 illustrates a strong upward trend in recent years. We believe this to be owing to better access to data and computing power, along with a growing awareness and access to data mining tools that are accessible to users outside of the data mining community. These tools include the Weka data mining software, which enables users to directly apply data mining algorithms to their data through Java interfaces or a graphical user interface [ 21 ].
Publications Per Country. The number of publications per country identified a predominance in the filed by European countries, the USA and China
Publications Per Year. Number of articles per year between January 2000 and October 2017. We identified an apparent tendency of an increased number of publications on data mining and epidemiology in recent years
Study objectives
The summary statistics for the study objectives are as follows: sixty percent of the study objectives were to forecast or predict epidemiological values/outcomes, such as the AQI or increases in emergency room visits. Thirty percent performed hypothesis generation. This included objectives, such as learning from the data, in which combinations of variables are associated with increases in hospitalization, and understanding which combination of meteorological variables are associated with a degradation in air quality due to emissions from neighbouring cities. Finally, ten percent of the studies focused on source apportionment.
Data mining paradigm
We identified that classification, regression, clustering and association mining algorithms have been applied. Classification and regression relate to prediction and forecasting objective, whereas clustering and association mining generally apply to hypothesis generation and source apportionment.
Table 4 includes the articles in a list sorted according to the objectives of the research. Data mining methods for performing numeric predictions, such as regression and classification, were most widely applied. This area encompassed 59% of the research. Clustering algorithms were applied in 26% of the work, and 15% of the articles employed association mining.
Detailed analysis
Source apportionment.
Table 5 summarizes source apportionment studies employing data mining techniques. These studies explore the impact of chemical emissions and other airborne agents in conjunction with climatological factors [ 22 – 24 ]. They focus on apportioning particular airborne pollutants to potential sources, such as industrial sites, regions and major intersections. These studies have mainly focused on outdoor and urban air pollution as it is the most widely known issue. In particular, principal component analysis (PCA) has been applied to identify correlations and the importance of particular meteorological parameters, traffic, fuel fired equipment and industries in causing air pollution [ 23 – 25 ]. Alternative approaches have utilized clustering-based solutions with correlation analysis to accomplish the task of source apportionment [ 22 , 23 ].
Strengths : The work presented in [ 23 ] proposes to perform enhanced source apportionment and classification. The authors claim that the key to achieving this is in the use of clustering algorithms developed for data mining. The advantage of these is that they are intended for rich, high-dimensional datasets that may include outliers. These factors can be problematic for conventional methods of source apportionment, such as principle component analysis and positive matrix factorization.
Once again, we have identified that the clarity with which the authors present the problem, and then juxtapose the limitation of conventional methods with the potential of data mining approaches, to be a very strong point in this paper. In addition, we appreciate that the authors have gone beyond simply applying standard clustering algorithms, and rather, employed their domain knowledge in order to refine the method in order to develop a superior clustering algorithm for the domain. The authors describe their algorithm, how to set the threshold parameter and the data pre-processing in detail. Crucially, this makes the proposed solution easily implementable by others.
Forecasting and prediction
Tables 5 and 6 summarizes 18 studies which applied machine learning techniques. We observed that investigators are primarily interested in predicting a) the distribution of ambient pollutant concentrations or related measures such as the air quality index (AQI), b) human exposure or c) risk of a health outcome.
According to the above points, the first category consists of 15 studies which either focus on predicting the distribution of particular air pollutants or predicting the quality of air in general. Twenty-seven percent of the above 15 studies (i.e. 4) focus on predicting or forecasting the air quality or air pollution in general. Sixty-six percent of the studies (i.e. 10) are interested in well-known specific air pollutants such as nitrogen oxides (NOx), particulate matter (PM), sulfur dioxide (SO2), carbon monoxide (CO), ozone (O3) and Volatile Organic Compounds VOCs. An interesting, and potentially fruitful, data source utilized by some of the studies that focus on air quality prediction comes from social media posts; social media offers a very rich source of information, which is not typically utilized in scientific analyses of this type [ 26 , 27 ].
Fifty percent of the studies focusing on specific air pollutants use artificial neural networks. Other well-known data mining techniques used include decision trees and support vector machines. In addition, some studies have used ensemble models which are composed of multiple models. The final outcome is determined based on the consensus of the outcome of each model, or some other method of arbitration. Ensemble models have been demonstrated to outperform the base classifiers from which they are composed in a variety of settings. They can be applied to both discrete and continuous value prediction [ 28 , 29 ].
The second category, namely human exposure, consists of 4 studies. These studies focus on identifying regions or exposures, predicting the activities of humans to help understand the exposure better and quantifying the exposure levels.
Interestingly, some of the studies also focus on building better infrastructure to collect data, or on ways to improve the quality of the collected data. This investment can be interpreted as a level of confidence in the application of data mining, and its potential to help shape future research and understanding. The interest in more fundamental problems like data collection and the accuracy of the collected data, in addition to a single focus on building a model based on the available data is very important. Work based on primary questions as such these will ensure high-quality datasets are available in the future, and thus, that better data mining and machine learning models will be possible.
Strengths : The authors in [ 30 ] propose a hybrid system that incorporates a variety of machine learning methods to produce more accurate forecasts and evaluations of air pollution. The authors note that data driven approaches are often more accurate and less complex than model-based approaches, such as chemical transport models, for predicting air quality. Data mining and machine learning-based approaches are data driven methods that are recognized as being powerful forecasting tools. This motivates them as a good choice for the authors. Although we do not see this as being as strong as the previous motivations for applying data mining and machine learning, it is certainly a sufficient reason to consider machine learning.
Hypothesis generation
We observed that many studies (i.e. above 60% of the studies that we have considered) have predominantly applied association rule mining—a primary class of data mining techniques—to generate new hypotheses regarding potential connections between air pollution and adverse health conditions.
From the identified articles, we observed that respiratory disease is an adverse health outcome of interest in these studies. Many studies focusing on respiratory disease are interested in finding out any potential connection between the disease and particulate matter or other airborne pollutants such as SO2 and NOx.
Our results demonstrated that there is a growing interest in generating new hypotheses explaining the connection between a combination of air pollutants and a particular adverse health impact. In [ 31 ], for exampled, the authors used the Bayesian Kernel Machine Regression (BKMR) method, which was recently introduced by epidemiologists. This illustrates the benefit of applying data mining methods to modern epidemiological datasets.
Strengths : The authors in [ 20 ] are interested in generating hypotheses about the joint effect of multiple airborne chemicals on pediatric asthma. Their work demonstrates that classification and regression trees can be used to overcome the challenge presented by multiple chemical interactions when identifying complex joint effects.
We have identified this as a noteworthy paper because the authors are studying a problem that is difficult to solve using conventional epidemiological methods. The paper is strengthened by the fact that the authors clearly justify the ML/DM solution to the problem. In addition, the authors explain why they selected the specific ML algorithm. Finally, this work is an excellent example of how ML/DM algorithms can be augmented and combined with knowledge and practices from the target domain in order to make an accurate and appropriate joint methodology. In particular, the authors demonstrate a refinement to the standard CART algorithm to control for confounding variables. This is important to note because in some applications, data mining practitioners can lose sight of useful, and often necessary, domain knowledge, which hampers the final results. Table 7 summarizes 15 studies which applied data mining techniques to generate new hypotheses to better understand the relationship between air pollution and health.
Challenges and limitations
We have identified a few reoccurring challenges in the surveyed papers. A major theme revolves around data. Many articles, for example, report results from data collected over a short period of time, and from one, or only a few, locations [ 32 , 33 ]. As a result, the findings cannot necessarily be generalized to new locations. This is particularly the case for prediction models trained on local data.
Most real-world data requires preprocessing to combine data sources, remove noise and properly structure the data. The necessities of this may be challenging for domain practitioners. Moreover, certain decisions that must be made during preprocessing can have an impact on the effectiveness of the trained model. Decision trees and association mining algorithms, for example, take categorical variable inputs, whilst continuous variables are common in epidemiology and atmospheric science. Thus, variables, such as temperature, must be converted to discrete categories (low, medium, high) for example [ 33 ]. In many cases, the ideal split points may be unclear. In general, the current literature does not focus on how to best preprocess air pollution epidemiological datasets.
Given the volume of social media data, and the fact that the vast majority of it is irrelevant to the data mining objective, it often has to be filtered. In [ 27 ], for example, keyword filtering is applied to gather relevant micro-blogs from Sina Weibo. How exactly to filter, or process the data, is an open question. A potential new direction here is to apply feature selection or feature extraction [ 2 ].
As noted by [ 34 ], it is important to recognize the limits of your data. Issues, such as granularity and representativeness, can limit what can be discovered from the data. Likewise, when generating association rules to predict outcomes, such as hospitalization or an increase in respiratory disease from weather and pollution data, the training data may not account for all relevant factors. In [ 35 ], it is noted that their data does not account for the accumulative nature of health outcomes.
Other challenges in applying data mining methods include the selection of user-specified parameters for the algorithms. Choosing the ideal number of clusters, for example, is important for performance of clustering algorithms [ 22 ]. In addition, metrics must be used that are appropriate for the target domain. In some cases, suitable evaluation metrics may not exist within the data mining literature, in which case new metrics may be required [ 36 ].
Finally, in many cases practitioners prefer data mining models that produce predictions in a manner that can be easily analyzed and understood [ 32 , 36 ]. This limits the choice of algorithms to rule learners and decision trees, and thus, many of the strongest algorithms are omitted. Perhaps, research focused on making the predictions of artificial neural networks and support vector machines more interpretable could be helpful for the health sciences community [ 37 ].
From an application perspective, we found the discussion of data mining related choices to be limited. Whilst the majority of the articles surveyed contain sufficient details about the algorithms implemented, readers could benefit from a similar level of detail in regards to other key design and implementation decisions. With few exceptions, such as [ 38 ], most of the surveyed articles report results for a single data mining algorithm. Readers would benefit from understanding how and why the specific choice of algorithm was made. As we noted in the overview section on Paradigms of Data Mining Algorithms, it is standard within the data mining community to run trials using a diverse set of algorithms. We often missed a discussion of details regarding which other algorithms were considered, and how they were evaluated. Finally, details regarding how the software was implemented and which data mining packages were used would be valuable to other readers from the air pollution epidemiology community.
Future directions
Deep learning.
Traditional artificial neural networks have proven to be accurate predictors for classification and regression problems. Within this survey, we have found them to be used for predicting global ground level PM 2.5 [ 4 ], predicting air pollution indicators and modeling personal exposure [ 39 ]. In recent years, however, deep learning has elevated the potential for learning with artificial neural networks to new heights. Thus, deep learning methods may also be very fruitful within air pollution epidemiology.
Deep learning is based on standard artificial neural network algorithms but utilizes much larger and deeper networks trained on big datasets. The training process in conjunction with the depth of the networks enables the learning of data abstractions at the different depths. This is found to disentangle complex features. Deep learning methods have been highly effective in areas such as image classification, speech recognition, and other complex problems [ 2 ].
Model selection
Model selection and evaluation are very important aspects of applying machine learning algorithms to real-world applications. However, they often receive less attention than the machine learning algorithms themselves. It is important to consider the breadth of techniques when developing applications in data mining in order to select the right approach for the domain.
For a given machine learning algorithm, model selection refers to the choosing of a parameterized version of the model based on the training data. The key is to select a model that will perform well on unseen data in the future. Once a parametrized model has been selected, the evaluation process provides an estimate of how the model will perform during future application. Some common evaluation metrics are accuracy, root mean square error (RMSE), f-measure and the area under the ROC curve (AUC).
Cross-validation
In the surveyed literature, various forms of cross validation have been applied [ 24 , 26 , 38 ]. In addition to these, various other methods can be applied, each of which has strengths and weaknesses. It is important to select a method that is appropriate for your target domain. Evaluation metrics estimate performance in different ways, and thus, it is important to choose one that is consistent with the target domain. The details of model selection and evaluation are thoroughly discussed in [ 6 ].
- Association mining
Our results demonstrated that much of the research that applied hypothesis generation utilize association mining. These studies typically relied on frequency to identify the associations. It is worth pointing out some alternatives, particularly for scientific domains. Statistical significance test-based methods, for example, have been developed to offer a better assessment of the quality of the association [ 40 , 41 ]. These could be of great benefit to future applications in air pollution epidemiology.
Class imbalance
In a related context, [ 38 ] noted the potential impact of class imbalance, or skewed class distributions, on the performance of machine learning algorithms. Class imbalance is said to occur when one class is significantly less likely, or less frequent, in the training set, than the other class. A detailed discussion of the impacts and potential solutions to class imbalance is undertaken in [ 42 ]. Given that we are often interested in less frequent, or even rare, events in air pollution epidemiology, methods developed for imbalanced learning may have great potential here.
Recent progress in technology and corresponding decreases in the price of computing power has made if possible to measure and store a wide variety of environmental health variables and form them into big datasets. Moreover, social media and other on-line resources provide an entirely new perspective from which to conduct environmental health analyses. These big datasets come with complexities that render it difficult to rely on traditional epidemiological or environmental health models to analyze them. To this end, data mining methods offer great potential to advance our understanding of the causes and impacts of air pollution.
From our survey, we have found a strong increase in the number of articles reporting to apply data mining methods to air pollution epidemiology. We attribute this to the increasing availability of large datasets and computing power, along with the growing awareness of the potential benefits of data mining. In spite of this trend and the potential benefit within the field, to the best of our knowledge, a survey of the existing state-of-the-art has not been performed.
To fill this void, we undertook a study to explore the extent to which data mining has been applied to air pollution epidemiology. This survey is intended for practitioners and researchers alike. We aim to point domain researchers to existing data mining applications within their respective areas, and related areas, as well as advance their understanding of the potential of data mining and inspire them to explore further research avenues.
Our survey illustrates that a wide variety of data mining algorithms have been applied to various sub-fields of air pollution epidemiology. Machine learning algorithms, for example, have been applied both as classifiers and regressors in forecasting and prediction problems. Clustering algorithms, such as K-Means and hierarchical clustering have been applied to knowledge discovery and source appropriation. In addition, a great number of studies have applied association mining for hypothesis generation.
1 see https://www.ncbi.nlm.nih.gov/pubmed
2 https://www.plos.org
3 https://scholar.google.ca
4 General refers to the study of air pollutants not specific to a certain setting.
Domingos P. A few useful things to know about machine learning. Commun ACM. 2012; 55(10):78–87.
Article Google Scholar
LeCun Y, Bengio Y, Hinton G. Deep learning. Nature. 2015; 521(7553):436–44.
Article CAS PubMed Google Scholar
Dietterich TG, et al. Ensemble methods in machine learning. Multiple Classif Syst. 2000; 1857:1–15.
Lary DJ, Faruque FS, Malakar N, Moore A, Roscoe B, Adams ZL, Eggelston Y. Estimating the global abundance of ground level presence of particulate matter (pm2. 5). Geospatial Health. 2014; 8(3):611–30.
Neto UMB, Dougherty ER. Error estimation for pattern recognition. Hoboken: John Wiley & Sons; 2015.
Book Google Scholar
Japkowicz N, Shah M. Evaluating Learning Algorithms: a Classification Perspective. Cambridge: Cambridge University Press; 2011.
Bellinger C, Amid A, Japkowicz N, Victor H. Multi-label classification of anemia patients. In: Proceedings of the IEEE 14th International Conference on Machine Learning and Applications (ICMLA).2015. p. 825–30.
Bishop C. Pattern Recognition and Machine Learning (Information Science and Statistics). 1613-9011. Cambridge: Springer; 2006.
Google Scholar
Breiman L, Friedman J, Stone CJ, Olshen RA. Classification and Regression Trees. Chicago: CRC Press; 1984.
Quinlan JR. Induction of decision trees. Mach Learn. 1986; 1(1):81–106.
Quinlan JR. C4. 5: Programs for Machine Learning. San Francisco: Morgan Kaufmann; 1993.
Rumelhart DE, Hinton GE, Williams RJ. Learning internal representations by error propagation. Parallel Distributed Processing: Exploration of the Micro-structure of Cognition. 1986; 1:1–34.
Maas AL, Hannun AY, Ng AY. Rectifier nonlinearities improve neural network acoustic models. In: Proceedings of the International Conference on Machine Learning.2013.
Vapnik V. The Nature of Statistical Learning Theory. New York: Springer; 1995.
Schölkopf B, Smola AJ. Learning with kernels. Cambridge: MIT Press; 2002.
Agrawal R, Srikant R. Fast algorithms for mining association rules. In: Proceedings of the 20th International Conference on Very Large Data Bases (VLDB).1994. p. 487–99.
Kitchenham B. Procedure for undertaking systematic reviews. Technical report, Computer Science Department, Keele University (TRISE-0401) and National ICT Australia Ltd (0400011T. 1), Joint Technical Report. 2004.
Moher D, Liberati A, Tetzlaff J, Altman D. Preferred reporting items for systematic reviews and meta-analyses: the prisma statement. J Clin Epidemiol. 2009; 62(10):1006–12.
Article PubMed Google Scholar
Runge-Ranzinger S, Horstick O, Marx M, Kroeger A. What does dengue disease surveillance contribute to predicting and detecting outbreaks and describing trends?Trop Med Int Health. 2008; 13(8):1022–41.
Gass K, Klein M, Chang HH, Flanders WD, Strickland MJ. Classification and regression trees for epidemiologic research: an air pollution example. Environ Health. 2014; 13(1):17.
Article PubMed PubMed Central Google Scholar
Hall M, Frank E, Holmes G, Pfahringer B, Reutemann P, Witten IH. The weka data mining software: An update. SIGKDD Explor Newsl. 2009; 11(1):10–18.
Chen HW, Tsai CT, She CW, Lin YC, Chiang CF. Exploring the background features of acidic and basic air pollutants around an industrial complex using data mining approach. Chemosphere. 2010; 81(10):1358–67.
Chen M, Wang P, Chen Q, Wu J, Chen X. A clustering algorithm for sample data based on environmental pollution characteristics. Atmos Environ. 2015; 107:194–203.
Article CAS Google Scholar
Singh KP, Gupta S, Rai P. Identifying pollution sources and predicting urban air quality using ensemble learning methods. Atmos Environ. 2013; 80:426–37.
Thurston GD, Spengler JD. A quantitative assessment of source contributions to inhalable particulate matter pollution in metropolitan boston. Atmos Environ (1967). 1985; 19(1):9–25.
Jiang W, Wang Y, Tsou MH, Fu X. Using social media to detect outdoor air pollution and monitor air quality index (aqi): a geo-targeted spatiotemporal analysis framework with sina weibo (chinese twitter). PloS ONE. 2015; 10(10):0141185.
Wang S, Paul MJ, Dredze M. Social media as a sensor of air quality and public response in china. J Med Internet Res. 2015; 17(3):22.
Freund Y, Schapire RE. Experiments with a new boosting algorithm. In: Proceedings of the Thirteenth International Conference on Machine Learning: 1996. p. 148–56.
Friedman JH. Greedy function approximation: a gradient boosting machine. Ann Stat. 2001; 29(5):1189–232.
Xu Y, Yang W, Wang J. Air quality early-warning system for cities in china. Atmos Environ. 2017; 148:239–57.
Bobb JF, Valeri L, Henn BC, Christiani DC, Wright RO, Mazumdar M, Godleski JJ, Coull BA. Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics. 2014; 16(3):058.
Payus C, Sulaiman N, Shahani M, Bakar AA. Association rules of data mining application for respiratory illness by air pollution database. Int J Basic Appl Sci. 2013; 13(3):11–16.
Kukkonen J, Partanen L, Karppinen A, Ruuskanen J, Junninen H, Kolehmainen M, Niska H, Dorling S, Chatterton T, Foxall R, et al. Extensive evaluation of neural network models for the prediction of no 2 and pm 10 concentrations, compared with a deterministic modelling system and measurements in central helsinki. Atmos Environ. 2003; 37(32):4539–550.
Reid CE, Jerrett M, Petersen ML, Pfister GG, Morefield PE, Tager IB, Raffuse SM, Balmes JR. Spatiotemporal prediction of fine particulate matter during the 2008 northern california wildfires using machine learning. Environ Sci Technol. 2015; 49(6):3887–96.
Zhu W, Wang J, Zhang W, Sun D. Short-term effects of air pollution on lower respiratory diseases and forecasting by the group method of data handling. Atmos Environ. 2012; 51:29–38.
Toti G, Vilalta R, Lindner P, Lefer B, Macias C, Price D. Analysis of correlation between pediatric asthma exacerbation and exposure to pollutant mixtures with association rule mining. Artif Intell Med. 2016; 74:44–52.
Setiono R, Liu H. Understanding neural networks via rule extraction. In: Proceedings of the International Joint Conference of Artificial Intelligence (IJCAI).1995. p. 480–5.
Pandey G, Zhang B, Jian L. Predicting submicron air pollution indicators: a machine learning approach. Environ Sci Process Impacts. 2013; 15(5):996–1005.
Aquilina NJ, Delgado-Saborit JM, Gauci AP, Baker S, Meddings C, Harrison RM. Comparative modeling approaches for personal exposure to particle-associated pah. Environ Sci Technol. 2010; 44(24):9370–6.
Hämäläinen W. Statapriori: an efficient algorithm for searching statistically significant association rules. Knowl Inform Syst. 2010; 23(3):373–99.
Hämäläinen W. Kingfisher: an efficient algorithm for searching for both positive and negative dependency rules with statistical significance measures. Knowl Inform Syst. 2012; 32(2):383–414.
He H, Ma Y. Imbalanced Learning: Foundations, Algorithms, and Applications. Piscataway: John Wiley & Sons; 2013.
Min KD, Kwon HJ, Kim K, Kim SY. Air pollution monitoring design for epidemiological application in a densely populated city. Int J Environ Res Public Health. 2017; 14(7):686.
Article PubMed Central Google Scholar
Keller JP, Drton M, Larson T, Kaufman JD, Sandler DP, Szpiro AA. Covariate-adaptive clustering of exposures for air pollution epidemiology cohorts. Ann Appl Stat. 2017; 11(1):93.
Li D, Liu J, Zhang J, Gui H, Du P, Yu T, Wang J, Lu Y, Liu W, Cheng Y. Identification of long-range transport pathways and potential sources of pm2.5 and pm10 in beijing from 2014 to 2015. J Environ Sci. 2017; 56:214–29.
Stingone JA, Pandey OP, Claudio L, Pandey G. Using machine learning to identify air pollution exposure profiles associated with early cognitive skills among u.s. children. Environ Pollut. 2017; 230:730–40.
Liu BC, Binaykia A, Chang PC, Tiwari MK, Tsao CC. Urban air quality forecasting based on multi-dimensional collaborative support vector regression (svr): A case study of beijing-tianjin-shijiazhuang. PLOS ONE. 2017; 12(7):1–17.
Mirto M, Fiore S, Conte L, Bruno LV, Aloisio G. A spatial data analysis infrastructure for environmental health research. In: Proceedings of the International Conference on High Performance Computing and Simulation (HPCS): 2016. p. 435–42.
Lewis AC, Lee JD, Edwards PM, Shaw MD, Evans MJ, Moller SJ, Smith KR, Buckley JW, Ellis M, Gillot SR, et al. Evaluating the performance of low cost chemical sensors for air pollution research. Faraday Discuss. 2016; 189:85–103.
Reid CE, Jerrett M, Tager IB, Petersen ML, Mann JK, Balmes JR. Differential respiratory health effects from the 2008 northern california wildfires: a spatiotemporal approach. Environ Res. 2016; 150:227–35.
Fernández-Camacho R, Cabeza IB, Aroba J, Gómez-Bravo F, Rodríguez S, de la Rosa J. Assessment of ultra-fine particles and noise measurements using fuzzy logic and data mining techniques. Sci Total Environ. 2015; 512:103–13.
Lary D, Lary T, Sattler B. Using machine learning to estimate global pm2. 5 for environmental health studies. Environ Health Insights. 2015; 9(Suppl 1):41.
CAS PubMed PubMed Central Google Scholar
Qin S, Liu F, Wang C, Song Y, Qu J. Spatial-temporal analysis and projection of extreme particulate matter (pm 10 and pm 2.5) levels using association rules: A case study of the jing-jin-ji region, china. Atmos Environ. 2015; 120:339–50.
Chen J, Chen H, Zheng G, Pan JZ, Wu H, Zhang N. Big smog meets web science: smog disaster analysis based on social media and device data on the web. In: Proceedings of the 23rd International Conference on World Wide Web. ACM: 2014. p. 505–10. http://www.sciencedirect.com/science/article/pii/S1352231015303484 .
Dias D, Tchepel O. Modelling of human exposure to air pollution in the urban environment: a gps-based approach. Environ Sci Pollut Res. 2014; 21(5):3558–71.
Philibert A, Loyce C, Makowski D. Prediction of n 2 o emission from local information with random forest. Environ Pollut. 2013; 177:156–63.
Padula AM, Mortimer K, Hubbard A, Lurmann F, Jerrett M, Tager IB. Exposure to traffic-related air pollution during pregnancy and term low birth weight: estimation of causal associations in a semiparametric model. Am J Epidemiol. 2012; 176(9):148.
Ma Y, Richards M, Ghanem M, Guo Y, Hassard J. Air pollution monitoring and mining based on sensor grid in london. Sensors. 2008; 8(6):3601–623.
Article CAS PubMed PubMed Central Google Scholar
Niska H, Hiltunen T, Karppinen A, Ruuskanen J, Kolehmainen M. Evolving the neural network model for forecasting air pollution time series. Eng Appl Artif Intell. 2004; 17(2):159–67.
Kolehmainen M, Martikainen H, Ruuskanen J. Neural networks and periodic components used in air quality forecasting. Atmos Environ. 2001; 35(5):815–25.
Challoner A, Pilla F, Gill L. Prediction of indoor air exposure from outdoor air quality using an artificial neural network model for inner city commercial buildings. Int J Environ Res Public health. 2015; 12(12):15233–53.
Pegoretti S, Verdi L. Machine learning for the analysis of indoor radon distribution, compared with ordinary kriging. Radiat Prot Dosim. 2009; 137(3-4):324–8.
Bell SM, Edwards SW. Identification and prioritization of relationships between environmental stressors and adverse human health impacts. Environ Health Perspec. 2015; 123(11):1193–9.
Bell SM, Edwards SW. Building associations between markers of environmental stressors and adverse human health impacts using frequent itemset mining. In: Proceedings of the SIAM International Conference on Data Mining: 2014. p. 551–9.
Hu M, Li W, Li L, Houston D, Wu J. Refining time-activity classification of human subjects using the global positioning system. PloS ONE. 2016; 11(2):0148875.
Beckerman BS, Jerrett M, Martin RV, van Donkelaar A, Ross Z, Burnett RT. Application of the deletion/substitution/addition algorithm to selecting land use regression models for interpolating air pollution measurements in california. Atmospheric Environ. 2013; 77:172–7.
Dominici F, Peng RD, Bell ML, Pham L, McDermott A, Zeger SL, Samet JM. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. Jama. 2006; 295(10):1127–34.
Corani G. Air quality prediction in milan: feed-forward neural networks, pruned neural networks and lazy learning. Ecol Model. 2005; 185(2):513–29.
Ghanem M, Guo Y, Hassard J, Osmond M, Richards M. Sensor grids for air pollution monitoring. In: Proc. 3rd UK e-Science All Hands Meeting.Nottingham: 2004.
Download references
Acknowledgments
The authors are grateful for the financial support of CIHR/NSERC.
This work was supported by a Collaborative Health Research Grant for CIHR/NSERC, and the Alberta Institute for Machine Intelligence (AMII).
Availability of data and materials
The datasets generated or analyzed during our survey are available from the corresponding author upon reasonable request.
Author information
Authors and affiliations.
Department of Computing Science, University of Alberta, Edmonton, Canada
Colin Bellinger, Mohomed Shazan Mohomed Jabbar & Osmar Zaïane
Department of Paediatrics, University of Alberta, Edmonto, Canada
Alvaro Osornio-Vargas
You can also search for this author in PubMed Google Scholar
Contributions
CB and MSMJ performed the literature review and gather the data used in this survey. CB and MSMJ performed the initial analysis and paper verification. All authors took part in the final analysis of the articles selected for inclusion in this survey. AOV examined and summarized the objectives of the surveyed articles from a biomedical perspective. Based on this analysis, OZ, CB and MSMJ designed the outline and structure of the survey. CB and MSMJ wrote the paper. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Colin Bellinger .
Ethics declarations
Ethics approval and consent to participate.
Not applicable.
Consent for publication
Competing interests.
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License( http://creativecommons.org/licenses/by/4.0/ ), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated.
Reprints and permissions
About this article
Cite this article.
Bellinger, C., Mohomed Jabbar, M., Zaïane, O. et al. A systematic review of data mining and machine learning for air pollution epidemiology. BMC Public Health 17 , 907 (2017). https://doi.org/10.1186/s12889-017-4914-3
Download citation
Received : 26 April 2017
Accepted : 14 November 2017
Published : 28 November 2017
DOI : https://doi.org/10.1186/s12889-017-4914-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Epidemiology
- Air pollution
- Data mining
- Machine learning
BMC Public Health
ISSN: 1471-2458
- General enquiries: [email protected]

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Reprod Biol Endocrinol
Air pollution and female fertility: a systematic review of literature
Alessandro conforti.
1 Dipartimento di Neuroscienze, Scienze Riproduttive ed Odontostomatologiche, Sezione di Ginecologia ed Ostetricia, Centro di Sterilità Università “Federico II” di Napoli, Naples, Italy
Marika Mascia
Giuseppina cioffi, cristina de angelis.
2 I.O.S. & COLEMAN Srl, Naples, Italy
3 Dipartimento di Medicina Clinica e Chirurgia, Sezione di Endocrinologia, Centro di Andrologia, Medicina della Riproduzione e della Sessualità Maschile e Femminile, Università “Federico II” di Napoli, Naples, Italy
Giuseppe Coppola
Pasquale de rosa, rosario pivonello, carlo alviggi.
4 Centro nazionale delle ricerche, Istituto per l’Endocrinologia e l’Oncologia Sperimentale (IEOS), Naples, Italy
Giuseppe De Placido
Associated data.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Air pollution is a cause of concern for human health. For instance, it is associated with an increased risk for cancer, cardiovascular and respiratory disorders. In vitro and in vivo studies suggested that air pollutants could act as endocrine disruptors, promote oxidative stress and exert genotoxic effect. Whether air pollution affects female infertility is under debate. The aim of the present study was to conduct a systematic review of studies that evaluated the impact of air pollution on female infertility. We systematically searched the MEDLINE (PubMed) and SCOPUS databases to identify all relevant studies published before October 2017. No time or language restrictions were adopted, and queries were limited to human studies. We also hand-searched the reference lists of relevant studies to ensure we did not miss pertinent studies. The risk of bias and quality assessment of the studies identified were performed using the Newcastle-Ottawa Scale. Primary outcomes were conception rate after spontaneous intercourse and live birth rate after in vitro fertilization (IVF) procedures. Secondary outcomes were first trimester miscarriage, stillbirths, infertility, number of oocytes and embryo retrieved. Eleven articles were included in the analysis. We found that in the IVF population, nitrogen dioxide and ozone were associated with a reduced live birth rate while particulate matter of 10 mm was associated with increased miscarriage. Furthermore, in the general population, particulate matter of 2.5 mm and between 2.5 and 10 mm were associated with reduced fecundability, whereas sulfur dioxide , carbon monoxide and nitrogen dioxide might promote miscarriage and stillbirths. The main limitation of our findigns resides in the fact that the desegn of studies included are observational and retrospective. Furthermore, there was a wide heterogenity among studies. Although larger trials are required before drawing definitive conclusions, it seems that air pollution could represent a matter of concern for female infertility.
Electronic supplementary material
The online version of this article (10.1186/s12958-018-0433-z) contains supplementary material, which is available to authorized users.
Introduction
Female infertility has increased in recent years [ 1 ]. It was estimated that this condition affects 1 in seven couples in developed countries [ 2 ]. Most cases of female infertility are related to specific disorders, namely, ovulatory disorders, endometriosis, chromosomal abnormalities and male factors [ 3 – 7 ]. There is also evidence that air pollutant could play a role in the pathogenesis of female infertility [ 8 – 10 ]. Air pollution appears to be a cause of concern for human health. For instance, it has been associated with an increased risk of cancer [ 11 ], and cardiovascular [ 12 ] and respiratory disorders in adults and children [ 13 , 14 ]. In addition, air pollutants have been associated with adverse perinatal outcomes [ 15 , 16 ].
Anthropogenic activities, namely traffic, industrial facilities and combustion of fossil fuels, which are particularly intense in large cities and in proximity of farms, are the main sources of health-related air pollutants. Air pollutants are in four main categories: gaseous pollutants (sulfur dioxide [SO 2 ], nitrate oxide [NO 2 ] and carbon monoxide [CO]), organic compounds (organic solvents or dioxins), heavy metals (lead and copper) and particulate matter (PM 10 PM 2.5-10 and PM 2.5 ) [ 17 ]. Ingestion and inhalation are the most common routes of exposure [ 17 ]. Ingestion is also facilitated by the fact that air pollution contributes to the contamination of food and water [ 18 ]. Some air pollutants, namely Cu, Pb and diesel exhaust seem to exert endocrine activity [ 19 ] that could affect female reproduction. Moreover, these endocrine “disruptors” exert estrogenic, antiestrogenic and antiandrogenic activity and some could interfere with the thyroid axis and influence metabolic disorders, such as insulin resistance and obesity, which are strictly related to infertility [ 20 – 22 ]. The increase in female infertility seems to parallel the increase in toxic emissions, which suggests that the impact of air pollution on human health could increase in the next years [ 23 , 24 ]. In an attempt to summarize current evidence, we carried out a systematic review of studies devoted to the impact of air pollutions on female infertility.
Material and methods
Protocol and eligibility criteria.
The present study was exempt from institutional and ethics board approval because it did not involve human intervention. We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [ 25 ]. The selection criteria are described according to PICO (Patients, Intervention, Comparison, and Outcomes). In detail, we evaluated fertility outcomes in women on reproductive age (in the general and IVF populations) in relation to exposure to air pollutants (Additional file 1 : Table S1).
Search strategy
We conducted a systematic search using MEDLINE (PubMed) and SCOPUS databases to identify all relevant studies published before October 2017. Combinations of the following keywords and MESH search terms were used: “air pollutants” AND (“miscarriage” OR “embryo” OR “pregnancy” OR “IVF OR “fecundability” OR “infertility” OR “menstrual disorders”). No time or language restrictions were adopted, and queries were limited to human studies. We also hand-searched reference lists of relevant studies to ensure we did not miss pertinent studies.
Selection of studies
Four reviewers (G.C., M.M., G.CO and P.D.) independently evaluated titles and abstracts. Duplications were removed using Endnote online software and manually. Disagreements were resolved by discussion with a third authors (A.C. and C.D.), and if required, with the involvement of the most experienced authors (R.P.,C.A., G.D.). Articles were included only if they appeared in peer-reviewed journals. Case series, case reports, book chapters, congress abstracts and grey literature [ 26 ], which includes a range of documents not controlled by commercial publishing organization, were not included.
Data extraction
Data were extracted independently by four reviewers (G.C., M.M., G.CO and P.D.) using predefined data fields, including study quality indicators. Discrepancies were resolved by discussion with the senior authors (R.P., C.A. and G.D.).
Risk of bias, summary measures and synthesis of the results
The risk of bias and quality assessment of the included studies were performed adopting the Newcastle-Ottawa Scale (NOS) [ 27 ]. Four authors (A.C, C.D., G.C. and P.D.) independently assessed the risk bias for each study. The senior authors (R.P., C.A. and G.D.) resolved conflicts. The NOS score was used to evaluate the studies included, and judgment on each one was passed according to three issues: selection of the study group, comparability between groups, and ascertainment of exposed/not exposed cohorts. Primary outcomes were conception rate after spontaneous intercourse and live birth rate after IVF procedures. Secondary outcomes were first trimester miscarriage, stillbirths, infertility, number of oocytes retrieved and embryos transferred.
Study selection and characteristics
A total of 4687 items were identified (Pubmed 2834 and Scopus 1853). A total of 2013 duplicates were removed manually and using the EndNote online library. The titles and abstracts of 2674 papers were scrutinized and 21 full papers were assessed for eligibility. Ten papers were excluded because they did not fulfill the inclusion criteria. Eleven articles were included in the analysis (Fig. 1 ). The characteristics of the studies included in the present study are reported in Table 1 .

Characteristics, findings and risk of bias of included studies
| Author, Year, (ref) | Study design | Population Country Individuals | Pollutants | Exposure | Confounders adjusted for | Significant effect size: | Effect size | 95% CI | NOS | |
|---|---|---|---|---|---|---|---|---|---|---|
| Dejmek et al. (2000) [ ] | Retrospective cohort | Czech Republic | 2585 (General population) | SO2 | Monitoring station obtained from by US EPA (Air Quality System) | Maternal age; parity; conception; seasonality; currently married; temperature average; temperature maxima; signal; year; season; epidemiological situation | Conception in the first unprotected menstrual cycle | OR = 0.57 SO2 levels (40-80 μg/m ) | 0.37–0.88 | 7 |
| OR = 0.49 SO2 levels (≥ 80 μg/m ) | 0.29–0.81 | |||||||||
| Sallmen et al. (2008) [ ] | Retrospective cohort | Portugal | 406 (General population) | Solvents used in shoe manufacturing (N-hexane and hexane isomers; Toluene; Methyl ethyl ketone; Acetone; Ethyl acetate; dichloromethane) | Air sampling was performed in the personal breathing zones of the exposed women, spanning roughly an 8-h work shift. | Female age; Last method of contraception; Age at menarch; Regularity of menstrual cycle; Male smoking; Female and male use of alcohol; Male exposure to metal dusts or fumes; Male exposure to engine exhausts. | Fecundability density ratio (low exposure to solvents) | FDR = 0.55 | 0.40–0.74 | 7 |
| Fecundability density ratio (high exposure to solvents) | FDR = 0.70 | 0.52–0.94 | ||||||||
| Green et al. (2009) [ ] | Prospective cohort | USA | 4979 (General population) | Traffic pollutants: NO2; O3; PM 2.5; PM 10, CO2 CH4, CO, H2S, NMHC NMOC; SO2; sulphur; THC | Traffic exposure were constructed using annual average daily traffic (AADT) counts near each residence and distance from residence to major roads | Maternal age, race, employment status, stressful life events and maternal smoking | Spontaneous abortion Maximum daily traffic within 50 m | 7 | ||
| > 90 centile | OR = 1.18 | 0.87–1.60 | ||||||||
| > 90 centile (African American) | OR = 3.11 | 1.26–7.66 | ||||||||
| > 90 centile (non smokers) | OR = 1.47 | 1.07–2.04 | ||||||||
| Mohorovic et al. (2010) [ ] | Prospective cohort | Croatia | 260 (General population) | Coal combustion (NO2; CO2; CO; other products) | Monitoring station (Labin meteorological station) | Crude data | Spontaneous abortion | OR = 2.99 | 0.91–9.80 | 5 |
| Perin et al. (2010) [ ] | Retrospective cohort | Brazil | 348 (IVF women) | PM10 | PM10 concentrations taken from 14 monitoring stations categorized into quartiles (Q1-Q4). | Ovarian response patterns to gonadotrophins, exposure, patient’s age, and the year of IVF treatment | Miscarriage in IVF women (> 56.72 µg/m3) | OR = 5.05 | 1.04–25.51 | 8 |
| Live birth rates (> 56.72 µg/m3) | OR = 1.71 | 0.72–4.09 | ||||||||
| Perin et al. (2010) [ ] | Retrospective cohort | Brazil | 177 (IVF women) 354 (General population) | PM10 | PM10 concentrations taken from 14 monitoring stations categorized into quartiles (Q1-Q4). | Ovarian response patterns to gonadotrophins, exposure, patient’s age, and the year of IVF treatment | Miscarriage in general population (> 56.72 µg/m3) | OR = 2.72 | 1.51–4.89 | 7 |
| Miscarriage in IVF women (> 56.72 µg/m3) | OR = 2.32 | 1.00–5.43 | ||||||||
| Legro et al. (2010) [ ] | Retrospective cohort | USA | 7403 (IVF women) | PM2.5 PM10 SO2 NO2 O3 | Monitoring station obtained from by US EPA (Air Quality System) | Age, IVF center and the year and season of oocyte retrieval | Live Birth Rate NO2 (after embryo transfer) O3 (after embryo transfer : | OR = 0.76 OR = 0.62 | 0.66–0.86 0.48–0.81 | 9 |
| Pregnancy rate PM2.5 (during embryo culture) | OR = 0.94 | 0.82–0.99 | ||||||||
| Faiz e al. (2012) [ ] | Retrospective cohort | USA | 343,077 (General population) | PM 2.5 SO2 NO2 CO | Central monitoring station monitored by Agency Air Quality System | Maternal age; Race/Ethnicity; Educational level; Prenatal care; Smoking; Neighborhood socioeconomic status; Calendar year; month of conception and; mean temperature | Stillbirths NO2 (first trimester) SO2 (first trimester) CO (second trimester) | OR = 1.16 OR = 1.13 OR = 1.14 | 1.03–1.31 1.01–1.28 1.06–1.24 | 8 |
| Slama et al. [ ] | Retrospective cohort | Czech Republic | 1916 (General population) | SO2, PM2.5, NO2, O3, carcinogenic PAHs | Central monitoring station | Maternal age, smoke habits and alcohol consumption before pregnancy,maternal education, marital status, BMI | Fertility rate PM2.5 NO2 | FR = 0.78 FR = 0.72 | 0.65–0.94 0.53--0.97 | 9 |
| Nieuwenhuijsen et al. (2014) [ ] | Cross-sectional | Spain | not available (General population) | PM10 PM2.5 PMcoarse fraction NO2 NOx O3 PM2.5 adsorbance | Land use regression developed in the European Study of Cohorts for Air Pollution Effects | Socioeconomic status, ethnicity, age, educational level | Fertility rate PM coarse fraction | FR = 0.88 | 0.83–0.94 | 7 |
| Mahalingaiah et al. (2016) [ ] | Prospective cohort | USA | 36,294 (General population) | PM 10, PM 2.5, PM 2.5–10 | USEPA Air Quality System | Age, smoking status, Race, BMI, parity, rotation shift work, oral contraception use, diet, Census tract level median income and median home value | Hazard ratio of primary and secondary infertility Living closer a major roads | HR = 1.11 | 1.02–1.20 | 9 |
Risk of bias
The risk of bias was evaluated with the NOS score and is reported in Table 1 .
Summary of results
We summarized our findings considering per each pollutant both IVF women and reproductive age women in general population (Table 2 ).
Synthesis of results
| Type of Pollutant | Population | Effect |
|---|---|---|
| NO | IVF | Lower live birth rates |
| General population | Higher miscarriage rate | |
| CO | General population | Higher stillbirth in second and third trimester |
| O | IVF | Lower live birth rates |
| PM | IVF | Lower pregnancy rates |
| General population | Reduced fecundability ratio | |
| PM | IVF | Higher miscarriage rate |
| General population | Higher miscarriage rate | |
| PM | General population | Reduced fertility rate |
| SO | IVF | No effect |
| General population | Higher early miscarriage and third trimester still births. Reduced conception rate | |
| Traffic pollutants | General population | Higher miscarriage rate; Higher infertility rates. |
| Coal combustion products | General population | Higher trend of miscarriage |
Increases in NO 2 concentrations were significantly associated with a lower live birth rate especially from embryo transfer to pregnancy test (OR 0.76, 95% CI 0.66–0.86, per 0.01 ppm increase) [ 28 ]. No effect on the number of oocytes retrieved or embryo transferred was observed [ 28 ].
General population
In a cross-sectional study involving women of reproductive age between 15 and 40 years, the fertility rate was not significantly associated with NO 2 exposure (OR 0.97, 95% CI 0.94–1.003) [ 9 ]. In contrast, another retrospective cohort study, showed that there was a significant decreased fecundability ratio per each increase of 10 μg/m 3 NO 2 exposure (OR 0.72, 95% CI 0.53–0.97) [ 29 ]. Miscarriage rate was significantly increased in women exposed to NO 2 compared to not exposed group (OR 1.16, 95% CI 1.01–1.28, per each 10-ppb increase in NO 2 concentration) [ 30 ].
Exposure to CO was significantly associated with stillbirth in the second (OR = 1.14, 95% CI: 1.01, 1.28) and third trimester (OR = 1.14, 95% CI: 1.06, 1.24) [ 30 ]. No significant association with first trimester miscarriage was reported (OR = 1.14, 95% CI 0.98, 1.32) [ 30 ].
A detrimental effect was observed in terms of live birth rate in women exposed to O 3 from embryo transfer to date of live birth (OR 0.62, 95% CI 0.48–0.81, per 0.02 ppm increase) [ 28 ]. No effect on the number of oocytes retrieved or embryo transferred was observed [ 28 ].
Only one study assessed the fecundability rate in the general population but no difference was reported between exposed and unexposed group [ 29 ].
Exposure to PM 2.5 during embryo culture was associated with a decreased conception rate (OR 0.90, 95% CI 0.82–0.99, per 8 μg/m 3 increase) but not with live birth rates [ 28 ]. No effect on the number of oocytes retrieved or embryo transferred was observed [ 28 ].
Multivariate hazard ratio (HR) analysis did not reveal any association with infertility considering 2 years average exposure (HR 1.09, 95% CI 0.77–1.55), 4 years average exposure (HR 0.91, 95% CI 0.78–1.05) and cumulative average exposure (HR 1.05, 95% CI 0.93–1.20) [ 8 ]. Consistently, in another trial multivariate analysis did not reveal any association with fertility rate [ 9 ]. On the other hand, The adjusted fecundability ratio was significantly decreased with each increase of 10 units (0.78, 95% CI 0.65–0.94) [ 29 ]. No statistically significant difference was observed in terms of late (second and third trimester) or early miscarriage (first trimester) [ 30 ].
PM 2.5–10
Multivariate HR analysis did not reveal any association between infertility and PM 2.5–10 considering 2-year average exposure (HR 1.10, 95% CI 0.98–1.23), 4 year average exposure (HR 1.05, 95% CI 0.93–1.19) and cumulative exposure (HR 1.10, 95% CI 0.99–1.22) [ 8 ]. Conversely, another study reported a significant reduction of spontaneous fertility rate in women exposed to PM 2.5–10 (incidence risk ratio: 0.88, 95% CI 0.84, 0.94) [ 9 ].
No significant effect was observed in terms of live birth rate, number of oocytes retrieved or embryos transferred in exposed women undergoing their first IVF cycle [ 28 ]. Furthermore, no significant effect was observed in the amount of gonadotropin used, number of oocytes retrieved, number of MII oocytes, embryo quality, clinical and live birth rate [ 26 , 31 ]. A higher risk of miscarriage was observed in women with a higher exposure to PM 10 (> 56.72 μg/m 3 ) comparing with those exposed to lower amount of PM 10 (≤ 56.72 μg/m 3 ) (OR 5.05 95% CI 1.04–25-51) [ 31 ].
Multivariate adjusted HR analysis per year did not reveal any association with infertility considering 2 years average exposure (HR 1.04, 95% CI 0.96–1.11), 4 years average exposure (HR 0.99, 95% CI 0.91–1.08) and cumulative average exposure (HR 1.06, 95% CI 0.99–1.13) infertility [ 8 ]. Multivariate incidence risk (IRR) ratio adjusted did not reveal any association between PM 10 exposure and fertility rate (IRR 0.99, 95% CI 0.96–1.02) [ 9 ]. A significant association with early miscarriage was observed in women exposed to over 56.72 µg/m3. [ 32 ].
Exposure to SO 2 did not significantly affect birth rate, number of oocytes retrieved or embryos transferred in women undergoing their first IVF cycle [ 28 ].
No differences in terms of adjusted fecundability rate was observed per an increase of 10 units in the SO 2 pollutant levels [ 29 ]. Conversely, in another study, the fecundability in the first unprotected menstrual cycle was significantly reduced only in couples exposed in the second month before conception to the following SO2 levels: 40–80 μg/m 3 (OR 0.57, 95% CI 0.37–0.88); ≥ 80 μg/m 3 (OR 0.49, 95% CI 0.29–0.81) [ 33 ]. The adjusted odds of miscarriage were significantly associated to SO 2 exposure (OR 1.13, 95% CI 1.01–1.28 per each 3 ppb increase in concentration) [ 30 ].
Organic solvents
Female exposure to air contaminated with organic solvents (hexane and hexane isomers, toluene, methyl ethyl ketone, acetone, ethyl acetate, isopropyl alcohol and dichloromethane, n-hexane, hexane isomers and toluene) was associated with reduced fecundability density ratio (FDR = 0.55, 95% CI 0.40–0.74) for low exposure (exposure index 0.01–0.14), and for high exposure (exposure index > 0.14), (FDR = 0.70, 95% CI 0.52.0.94). Moreover, exposure for less than 6 years was more strongly associated with reduced FDR in both low (FDR = 0.50, 95% Cl 0.30 to 0.83) and high exposure groups (FDR = 0.50, 95% CI 0.28–0.90) [ 34 ].
Traffic pollutants
In a large cohort study involving 4979 women, traffic pollutants were associated with an increased but not with significant risk of miscarriage rate among women exposed to a maximum annual average of traffic pollutants within 50 m (AOR 1.18 95%, CI 0.87–1.60). A significant association was observed in a subgroup analysis involving African Americans (AOR = 3.11; 95% CI, 1.26–7.66) and nonsmokers (AOR = 1.47; 95% CI, 1.07–2.04) [ 35 ]. In another large cohort study, women living closer to a major road had a higher risk of infertility than did women living far from a major road (HR, 1.11 95% CI: 1.02–1.20) [ 8 ].
Coal combustion pollutants
In a small prospective study of 260 women, the miscarriage rate was higher, albeit not significantly, in women exposed to coal combustion pollutants than in non-exposed women (OR 2.99, 95% CI 0.91–9.80) [ 36 ] .
Only 11 studies have evaluated the potential effect of air pollutants on female reproduction.. In the IVF context, NO 2 and O 3 were associated with impaired live-birth rates. In addition, exposure to high levels of PM 10 (> 56.72 μg/m 3 ) resulted in an increased miscarriage rate after IVF procedures. Consistently, no study reported a significant effect on other quantitative (i.e. number of oocytes retrieved, number of embryos transferred, and consumption of gonadotropin) and qualitative (embryo quality, and number of MII oocytes) IVF outcomes [ 28 , 31 , 32 ]. In natural conception, reduced fecundability was associated with solvents and SO 2 [ 33 , 34 ]. Notably while abortion rate was associated with traffic pollutants [ 8 , 35 ], and in particular SO 2 and NO 2 [ 30 ], no clear relation to coal combustion pollutants emerged [ 36 ]. Contrasting findings between infertility and PM 2.5–10 were reported [ 8 , 9 ].
Only three retrospective studies evaluated the effects of air pollution on IVF [ 28 , 31 , 32 ]. Although Legro and colleagues studied a large IVF population, the heterogeneity of IVF protocols and the lack of information about male partners represent two important limitation factors [ 28 ]. Moreover, the two studies conducted by Perin et al., are limited by the fact that only one pollutant was investigated and by the low number of cases enrolled [ 31 , 32 ].
Eight studies have been conducted on the general population. Of the three prospective studies, the one by Mahalingaiah et al. is the largest (more than 36,000 patients) and has the highest qualitative NOS score [ 8 ]. The quality of evidence was lowest in the study by Mohorovic et al. as was the number of observations, and the authors did not report effect size for each air pollutant separately [ 36 ]. The same weakness emerges in the Green et al. paper, which however analyzed such important factors as work exposure, residential history and employment status of the population studied [ 35 ]. Of the five retrospective studies conducted to-date, the quality of evidence is highest in two large studies conducted by Faiz and colleagues [ 30 ] and by Slama and colleagues [ 29 ] demonstrating that air pollutants significantly affect fertility and stillbirths rates. The remaining three retrospective studies have several limitations, namely a paucity of data regarding the population studied [ 9 ], a low number of pollutant analyzed [ 33 ] and the methods adopted to assess exposure [ 34 ].
The relationship between air pollutants and spontaneous fertility was first observed in an animal model [ 37 ]. In detail, Mohallem et al. observed an increased implantation failure rate and a significant reduction of births in mice exposed to polluted city air compared to non-exposed mice [ 38 ]. Similarly, Veras et al. found significantly fewer antral follicles and a lower fertility index in mice exposed to traffic pollutants versus non-exposed mice [ 39 ].
The effect of air pollutants on human spermatogenesis has also been investigated [ 40 – 43 ]. The largest study, conducted by Hammoud et al., reported that PM 2.5 exposure negatively correlated with sperm morphology and motility [ 40 ]. The negative effect of particulate matter was confirmed in a recent prospective cohort study that identified a significant association between PM 10 and PM 2.5 and sperm chromosomal abnormalities (i.e. disomy Y and disomy chromosome 21) [ 44 ].
The mechanism underlying the effect of air pollutants on female fertility is still a matter of debate. Several pathogenetic mechanisms have been proposed. Firstly, it was hypothesized that air pollutants could mimic the effect of androgens and estrogens in humans [ 45 ]. These endocrine-disrupting properties could exert their effect by interacting with nuclear receptor, the estrogen or androgen repertory or by interacting with specific targets in cytosol thus resulting in activation of the /Ras/Erk pathway [ 46 ]. Others have suggested that air pollutants could promote oxidative stress and inflammatory processes [ 17 ]. In this sense, we recently demonstrated that the addition of anti-oxidant factors to ovarian stimulation could improve reproductive outcome in women with polycystic ovarian syndrome [ 47 ]. However, whether antioxidant products could mitigate the effect of air pollutants on IVF outcomes remains to be determined. Finally, it has been suggested that air pollutants could exert a genotoxic effect. For instance, increased sperm DNA fragmentation was associated with exposure to elevated air pollution levels (at or above the upper limit of US air quality standards) [ 48 ]. Furthermore, DNA methylation seems to be significantly influenced by air pollutants [ 49 ]. Indeed, in a recent study of 777 men, an increase in air pollutant concentrations was significantly associated with F3, ICAM-1, and TLR-2 hypomethylation, and IFN-γ and IL-6 hypermethylation [ 50 ].
Our review has several limitations. First, most of the studies included in our analysis are observational and retrospective, and hence more prone to bias. Second, exposure ascertainment was heterogeneous among studies. Most of the trials assessed air quality using a specific air monitoring station, others estimated exposure according to proximity to the potential source [ 8 , 35 , 36 ]. In addition, the reference levels of each pollutant varied significantly among studies. Lastly, the populations investigated as well as the definitions used to assess infertility and miscarriage were also heterogeneous. These factors render a meta-analytic and quantitative approach to this issue challenging.
In conclusion, our meta-analysis suggests there is a close association between female infertility and air pollution. However, a more robust meta-analytic approach is required before any definitive conclusion can be reached.
Additional file
Table S1. Selection criteria according to PICO questions. (DOCX 14 kb)
Acknowledgements
The authors would like to thank IVF Unit Federico II Staff.
The authors thank Jean Ann Gilder (Scientific Communication srl., Naples, Italy) for editing the text.
Availability of data and materials
Abbreviations.
| AOR | Adjusted Odds ratio |
| BMI | Body mass index |
| CO | Carbon monoxide |
| Cu | Copper |
| ERK | Extracellular Signal-regulated Kinase |
| F3 | Tissue factor |
| FDR | Fecundability density ratio |
| HR | Hazard ratio |
| ICAM-1 | Intercellular adhesion molecule 1 |
| IL-6 | Interleukin-6 |
| INF-γ | Interferon gamma |
| IRR | incidence risk ratio |
| NO | Nitrogen dioxide |
| NMHC | Non-Methane hydrocarbons |
| NMOC | Non-Methane organic compounds |
| NOS | Newcastle-Ottawa Scale |
| O | Ozone |
| OR | Odds ratio |
| Pb | Lead |
| PM | Particulate matter of 10 μm |
| PM | Particulate matter of 2.5 μm |
| PM | Particulate matter of 2.5–10 μm (coarse fraction). |
| RAS | Signal transducing protein |
| SO | Sulphur dioxide |
| SRC | Signal transducing protein tyrosine kinase |
| THC | Total hydrocarbons |
| TLR-2 | Toll-like receptor 2 |
Authors’ contributions
CA, RP, GP and AC conceived the study. AC drafted the first version. MM, GC, CD, GC and PD contributed to data search and quality assessment. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable (review of published papers).
Consent for publication
Competing interests.
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The impact of air quality on tourism: a systematic literature review
Journal of Tourism Futures
ISSN : 2055-5911
Article publication date: 27 March 2020
Issue publication date: 4 June 2021
Tourism may have important positive and negative economic, socio-cultural and environmental impacts. However, cultural and natural resources are also the base to the development of competitive destinations and changes in these resources can have an important impact on tourism development. Despite the considerable literature regarding the impacts of tourism, a limited number of studies examine the impact of the environment on tourism, specifically the impact of air quality (AQ). Therefore, this paper aims to review what is known about the impact of AQ on tourism demand, analysing the different methods and approaches used, as well as the results obtained.
Design/methodology/approach
A systematic literature review method was used to examine the state of the art in this topic and identify research gaps and new research directions. Only 26 papers were identified that examine the impact of AQ on tourism demand.
The majority of the studies were carried out in China and investigate the impact of AQ on tourism from the perspective of tourism demand. Both global (tourism demand) and individual (tourist perceptions) approaches have been used to investigate the impact of AQ on tourism.
Originality/value
This is the first systematic literature review on the impact of outdoor AQ on tourism demand. Moreover, this paper analyses the methods and approaches that have been used in the literature to examine the impact of outdoor AQ on tourism demand. The paper ends with a discussion on the identified research gaps concerning the influence of AQ on tourism development.
- Air quality
- Air pollution
- Systematic literature review
Eusébio, C. , Carneiro, M.J. , Madaleno, M. , Robaina, M. , Rodrigues, V. , Russo, M. , Relvas, H. , Gama, C. , Lopes, M. , Seixas, V. , Borrego, C. and Monteiro, A. (2021), "The impact of air quality on tourism: a systematic literature review", Journal of Tourism Futures , Vol. 7 No. 1, pp. 111-130. https://doi.org/10.1108/JTF-06-2019-0049
Emerald Publishing Limited
Copyright © 2020, Celeste Eusébio, Maria João Carneiro, Mara Madaleno, Margarita Robaina, Vítor Rodrigues, Michael Russo, Hélder Relvas, Carla Gama, Myriam Lopes, Vania Seixas, Carlos Borrego and Alexandra Monteiro
Published in Journal of Tourism Futures . Published by Emerald Publishing Limited. This article is published under the Creative Commons Attribution (CC BY 4.0) license. Anyone may reproduce, distribute, translate and create derivative works of this article (for both commercial and non-commercial purposes), subject to full attribution to the original publication and authors. The full terms of this license may be seen at http://creativecommons.org/licences/by/4.0/legalcode
1. Introduction
In the present era, one of the major motivations for travelling is to avoid the usual environment and seek a site with a pleasant location for releasing psychological stress and pressure ( Ritchie and Crouch, 2003 ). Therefore, environmental quality must be taken into account as an important factor in the decision-making process of potential tourists, as it can have a significant effect on the competitiveness of tourism destinations ( Zhang et al. , 2015 ; Becken et al. , 2017 ). However, the environment in some large tourism destination countries such as Egypt, China and India, is deteriorating with the progressive urbanization and industrialization. Beyond the “traditional” environmental problems such as garbage disposal and water pollution, the problem of haze pollution has risen in recent years, and air quality (AQ) has become a universal concern ( Chen et al. , 2017 ), now being incorporated into the wider category of environmental quality.
Ambient AQ should attract more academic attention than thermal comfort and the aesthetic dimension of the physical environment, as AQ is closely related to health risks ( Costa et al. , 2014 ). However, the existing literature places relatively low attention on the effects of AQ on tourism demand and the competitiveness of tourism destinations. Overall, the impacts of environmental and climate change issues on tourism have previously been discussed in several studies but few of them have focussed directly on the impacts of air pollution on the competitiveness of a tourism destination ( Saenz-de-Miera and Rosselló, 2013 ; Rossello-Nadal, 2014 ; Sajjad et al. , 2014 ). AQ also pertains to physical comfort, which is crucial to tourist experiences and has become a severe concern for human health. Medical evidence suggests that short and long-term exposures to ambient air pollution can engender a wide variety of acute and chronic health problems ( Seaton et al. , 1995 ; WHO, 2017). Moreover, AQ also affects aesthetic enjoyment, with people’s perception of reduced visibility, which is affected by the presence of particles and haze, which is being increasingly researched ( Rizzi et al. , 2014 ).
The objective of this paper is to review what is known and has been published, about the impact of outdoor AQ on tourism demand, using a systematic literature review method. To date, there is no literature review study on this topic. It is of note that the impact of tourism on AQ was also not addressed. This literature review aims to identify the geographical context, research methodologies used, researched subjects of the papers and the findings on the impact of AQ on tourism. This approach was adopted to provide contributions to guide future research, regarding which models should be used and what kind of data needs to be collected.
The paper is organized in various sections. In Section 2, the methodology used to select and analyse the papers is presented. In Section 3, the findings are reported, specifically the distribution of papers over time, among journals, subject areas, authorship and citations, the geographical contexts of the studies and the research methods used (data collection and data analysis methods), as well as the key results found. Finally, in Section 4, the main conclusions are summarized, research gaps are identified and some research questions are proposed to overcome these gaps.
2. Methodology
Several types of methodologies have been used in previous articles to conduct a literature review (e.g. systematic literature review, structured literature review, bibliometric analysis and systematic literature network analysis) ( Centobelli and Ndou, 2019 ; Comerio and Strozzi, 2019 ). The differences among these methodologies are mainly related to the research protocol used. In this paper, a systematic literature review is applied and the research protocol used encompasses two stages. First, a protocol was defined and put into practice to select the articles that will be analysed. Second, a content analysis of the articles selected was undertaken.
2.1 Articles selection
The protocol used to select the papers is reported in Figure 1 .
As presented in Figure 1 , the identification of the studies was carried out through a search on the Scopus database during January 2019, using the following search code – (“AQ” or “atmospheric emissions” or “air pollutants”) and (“tourism” or “visitor” or “tourist”) – in the article title, abstract and keywords without any restriction of time or subject. This database has been used in several previous studies ( Centobelli and Ndou, 2019 ; Comerio and Strozzi, 2019 ; Dann et al. , 2019 ) and is one of the largest databases of peer-reviewed literature (scientific journals, books and conference proceedings). A total of 488 records were obtained. Further, to include both scientific literature and “grey” literature, articles, reviews, articles in press and conference proceedings were selected. As a consequence of this first screening, the sample of records reduced to 383. Further, only documents written in English were selected. Papers written in other languages were excluded, given the complexities associated with translation. Based on this screening, 26 records were excluded.
Manual screening of the abstract titles and the abstracts of the 357 records was carried out by two authors (one specialized in AQ and the other in tourism) to verify if each paper was relevant to be included in this research. When the title and the abstract were not conclusive, the whole article was analysed. Concerning the inclusion criteria, it was decided to include both conceptual and empirical studies (qualitative and quantitative), where the influence of outdoor AQ on tourism demand of a tourism destination was analysed. Therefore, papers regarding the environmental impact of tourism on AQ and studies concerning indoor AQ of tourism attractions and facilities were excluded from this systematic literature review. A great number of documents only mention the topics of AQ and tourism in a superficial way, without an analysis of the impact of outdoor AQ on tourism demand. Consequently, only 20 papers were selected. To increase the sample of papers selected, two complementary searches were carried out on the Google Scholar database and Online Knowledge Library (b-on). From these analyses, only one additional paper was added. Further, the references of the 21 papers identified were analysed and 5 more papers were included in the sample. Consequently, a total of 26 papers were selected to be analysed in the second stage of this systematic literature review. This reduced number of papers clearly shows that this topic has been almost neglected in the literature, despite the great increase that the tourism industry has registered in the past few years and the increase in well-being and health concerns.
2.2 Articles analysis
The distribution over time;
Distribution by journal, scientific area and authorship; and
The distribution by the geographical context where the study was conducted.
The research methods (data collection and data analysis methods);
The dimensions of AQ and tourism demand investigated; and
The results obtained concerning the impact of outdoor AQ on the dimensions of tourism demand analysed.
This content analysis was complemented with an investigation of word frequencies (in title, abstract and keywords), using the Nvivo software, to identify, through word clouds, the terms most frequently used in this research field.
3. Findings
3.1 distribution of the papers over time.
A total of 26 papers were analysed. There seems to be a growing interest on the impact of outdoor AQ on tourism demand among researchers, as most of these papers were published in the past decade (88 per cent), mainly in 2017 and 2018 (12 and 42 per cent of the total set of papers were published in these years, respectively) ( Figure 2 ).
3.2 Journals, authorship and citations
There is a great variety among the authors of these papers. Almost all (98 per cent) wrote one paper and only Rob Law is the author of two. The papers are published in journals and conference proceedings of several areas, which reveals the relevance of this topic to different fields. However, there is a higher prevalence of papers in journals or proceedings from the field of “tourism, leisure and hospitality management” (38 per cent), with a notable contribution of “environmental science” (19 per cent), also having some papers published in journals or proceedings in the areas of “geography, planning and development” (8 per cent) and “health” or “medicine” (8 per cent) ( Table I ). It is important to notice that journals or proceedings can be related to more than one field, for example, environment and health. Papers have, on average, 7.2 citations in Scopus and 11.0 citations in Google Scholar. However, there is a high variation regarding citations, with many of the most recent papers (representing 19 per cent of the total) not yet having any citations in Scopus or Google Scholar, while 23 per cent have more than 20 citations in Scopus or in Google Scholar ( Table I ).
3.3 Geographical context
In terms of geographical areas, Figure 3 reveals that the spatial distribution of the published work addressing the impact of AQ on tourism is mainly focussed over the China and Southeast Asia regions.
China emerges as the country where most studies were conducted (about 42 per cent of the total), mainly in its capital (Beijing) with five specific studies focussed on this city (and not included in the six studies for China as a country shown in Figure 2 ). When other Asian countries are considered, the number of studies carried out in this region represents 58 per cent of the total studies analysed. Moreover, 16 per cent of the published studies were undertaken in the USA. A limited number of studies were conducted in European countries.
3.4 Most frequently used terms
The word clouds were generated through the qualitative analysis software NVivo 12, which allowed us to develop a word frequency query. To do so, this task separately analysed the word frequency in specific items of the mentioned papers, namely, the title, keywords and abstract. By default, the software automatically excludes the so-called “stop words”, which refer to conjunctions and/or prepositions and similar, which helped to substantially reduce the number of meaningless words. In each case, the words with a frequency equal to “1” were excluded, mainly because they may not be meaningful to the study objectives. Additionally, the following expressions, matching with the search terms used in the initial protocol, were also excluded: “AQ”, “atmospheric emissions”, “air pollutants”, “tourism”, “visitor” and “tourist”. To obtain more accurate results, the words were grouped according to the option “stemmed words”, which groups similar words such as “significant” and “significantly”.
Originally, the analysis generated 930 words in the case of the abstracts, 142 for the titles and 118 for keywords. By applying the above-mentioned filter, the final result was a total of 432, 31 and 38 words, respectively. Based on each list of frequencies, the software created the following word clouds ( Figure 4 ). Focussing on the top five of the most significant words, and as observed in Figure 4 , only the expressions “pollution” and “environmental” are common in the analysed lists. The words “impact”, “China” and “perceptions” also appear with high frequency in, at least, two of the three lists of frequencies and “parks” or “haze”, reflecting the common topics between the several considered studies.
3.5 Research methods
Most papers selected for this systematic review include empirical studies, only one is a literature review ( Zajchowski et al. , 2018 ). The literature review carried out by Zajchowski et al. (2018) differs from the one in the present paper, as it only focusses on the social and psychological effects of degraded AQ in and around parks and protected areas, and only analyses papers published in journals. In contrast, the analysis carried out in the present paper focussed, as already mentioned, on destinations, excluding specific attractions, but encompassed a wider range of documents, including papers published in conference proceedings. Only three papers – Hill et al. (2000) , Keiser et al. (2018) and Zhang et al. (2015) – are cited in the two literature reviews.
In this section, the methods used in the papers that include an empirical study to collect and analyse the data are described. It was considered useful to include a summary of the methodologies adopted to examine the influence of outdoor AQ on tourism. This would be helpful in future research to identify potential methodologies that may be used to assess this influence.
3.5.1 Type of data and data collection methods.
In terms of the type of data used, the observed sample of articles reviewed is well distributed between primary and secondary data ( Table II ). A total of 56 per cent of our sample used primary data. From these, 11 articles use questionnaires to explore the relationship between AQ and tourism. Only one study relies on interviews directed to tourists and two rely on experiments to extract primary data. The data sources used to collect secondary data correspond to diverse sources, which can be divided into quantitative data and online reviews. In total, 14 studies collect data from quantitative national and international sources to explore the AQ-tourism relationship and only two of the reviewed articles consider tourists’ online reviews as secondary source data. Moreover, some studies simultaneously use primary and secondary data sources to drive reliable conclusions, merging experiments or questionnaires with secondary data. At least Hipp and Ogunseitan (2011) , Jun-hui (2018) and Pant et al. (2018) simultaneously use primary and secondary data. To study visitors’ perceptions of AQ or to infer about the impact of air pollution on tourism, the joint use of questionnaires and evaluations collected from well-known travelling opinion surveys (such as in TripAdvisor; Saura et al. , 2018 ) can be particularly efficient and practical.
3.5.2 Data analysis methods.
Table IV presents a summary of the methodologies used by the authors considered in this literature review regarding the impacts of AQ on tourism. Most of the studies analysed use a quantitative analysis (92 per cent), while only 8 per cent (two studies) rely on qualitative analysis.
In terms of econometric methodologies, simple data analysis is the preferred method considering that it is complex/difficult to collect a long time series of data using questionnaires to build hypotheses and then test them. Even so, the content analysis could be another alternative when using qualitative data, but authors have only recently started using it ( Wu et al. , 2018 ; Saura et al. , 2018 ). When using quantitative data, Table IV shows that the most applied methods are those of ANOVA, linear regression analysis and panel data models. Simple descriptive statistics are used in 80 per cent of the studies analysed, where correlation analysis and t -tests are also commonly applied to explore data properties. The use of χ 2 tests and reliability analysis is less common.
More complex econometric models are used when authors use quantitative secondary data ( Tables II and III). These models allow having both a clearer picture of the quantitative impact of AQ on tourism and economic growth, as well as development at national and regional levels. The analysis suggests that using secondary data panel models and time series models (like VAR) allows for a more complete analysis of the relationship between AQ and tourism. Content analysis, which has not been used, can be used together with other methods to perform a more in-depth analysis of the influence of AQ on the tourism demand.
capture both static and dynamic interdependencies;
treat the links across units in an unrestricted fashion;
easily incorporate time variations in the coefficients and in the variance of the shocks;
account for cross sectional dynamic heterogeneities; and
use Granger causality and capture more complex correlation analysis.
Moreover, more qualitative studies should be carried out in this field to examine the influence of AQ on the behaviour and experiences of tourists. Table IV evidences the limitations, thus, far in terms of methodology analysis and provides valuable future research directions.
3.6 Variables used
3.6.1 dimensions of air quality..
The variables used in the various studies to measure AQ and its impact on tourism differ, essentially, between studies that examine the impact of AQ on visitors and studies that analyse the impact of AQ on global tourism demand. In the first group, a great number of studies use the perception of AQ and the perception of haze pollution ( Table IV ). In a smaller number of studies, visitor perception of the environmental risks, atmospheric contaminations, ozone depletion, fog and smog are analysed. Additionally, other studies use measurements of variables related to AQ rather than visitor perception such as the pollution standard index (PSI), days of haze, visibility, particulate matter (PM) and black carbon.
Articles that analyse the impacts of AQ on global tourism demand are no longer based on perception but quantitative AQ variables. Most studies are based on indices of air pollution (or AQ). There is another subset of studies that are based on emission variables (e.g. CO 2 , waste gases, methane, nitrous oxide and ozone). Moreover, there is a dispersion of studies that use other variables such as visibility, PM concentrations and haze.
3.6.2 Dimensions of tourism demand.
Individual visitors.
Global tourism demand.
In the first group, most of the studies examine the travel intention and destination choice. Moreover, the effect of AQ on tourism has also been analysed through the well-being and quality of life (QOL) variables (including physical and psychological health). A limited number of studies examined the impact of AQ on tourism experience, destination image, visitors’ satisfaction and type of activities carried out during a trip. In the second group, the studies focus on global tourism demand, mainly on the size of tourism flows (e.g. tourist arrivals, number of visitors, departures, international tourism receipts and expenditures) ( Table V ). However, several dimensions of tourism demand have been neglected in these studies such as the impact of AQ on destination competitiveness, emotions, memorability and post-travel behaviours.
3.7 Impact of air quality on tourism
Papers that analyse the impact of AQ on individual visitors.
Papers that examine the impact of AQ on global tourism demand.
3.7.1 Impact on individual visitors.
Travel behaviour, travel intention and destination choice;
Well-being and QOL;
Visitors’ satisfaction; and
Destination image.
3.7.1.1 Impact on travel behaviour, travel intention and destination choice.
A deep analysis of the results reveals that good AQ is likely to have a positive influence on travel behaviour, travel intention and destination choice ( Bohm and Pfister, 2011 ; Becken et al. , 2017 ; Hill et al. , 2000 ; Jun-hui, 2018 ; Law and Cheung, 2009 ; Zhang et al. , 2015 ; Zhu, 2018 ). This corroborates part of the findings of the literature review undertaken by Zajchowski et al. (2018) on the effects of good AQ on human behaviour. However, the variables representing AQ, the methodologies adopted and the tourism markets and destinations considered, vary across the studies. Zhu (2018) , Zhang et al. (2015) and Hill et al. (2000) analyse haze effects on tourism in Beijing, while Zhu (2018) examines how the haze affects the travel wishes and decisions of Beijing residents. The results show that for the majority of the residents, hazy weather has an impact on their willingness to travel and means of travel. More than 80 per cent of the respondents are not satisfied with travelling during fog and haze days. Moreover, differences in terms of age were identified, with young people (under the age of 20) being more reluctant to travel on haze days. Zhang et al. (2015) also analyse the potential impacts of haze pollution on the tourism industry of Beijing, through a questionnaire applied to potential tourists of this tourism destination. The results obtained reveal that haze pollution affects tourist choice of destinations and departure time. Differences are noticed among visitors with different travel purposes, with visitors travelling for sightseeing and leisure revealing a much higher concern regarding haze pollution than those travelling for business or visiting friends and relatives. Leading to visibility conditions that depend on haze affecting the likelihood of visiting the destinations in the future. Hill et al. (2000) analysed this topic for the White Mountain National Forest, NH (USA) and concluded that as visibility decreases, the probability of accepting visibility conditions tends to decrease and also that potential visitors planning a visit to the White Mountains in the future would be less likely to visit this protected area if the visibility conditions got worse. Finally, Jun-hui (2018) examines tourist perception of fog and haze in Xi’an (a world famous historical and cultural city in China). In this study, the tourists were categorized into three segments (“blunt type”, “normal type” and “sensitive type”) according to their perceptions of the fog and haze. Differences were obtained in terms of sociodemographic profiles and travel behaviour (before and during the trip). Tourists may not perceive the AQ conditions of the location they are visiting until they reach their home countries and feel the difference.
Other authors focussed on the tourist environmental risk perception and on the influence of this perception on present and future visits. Bohm and Pfister (2011) analyse traveller environmental risk perception in two tourism destinations with different environmental problems as follows: Australia (with ozone depletion) and Bangkok (with severe air pollution). Results show that travellers usually perceive lower risks than non-travellers, and that the decision to travel to environmentally afflicted destinations is related to people’s anticipated emotional response. Becken et al. (2017) also reveals that, to American and Australian citizens, feelings towards the air (affective risk perceptions) also have a negative impact on intentions to visit China. Law and Cheung (2009) concluded this when analysing international visitor perception of AQ (both indoor and outdoor) in Hong Kong. Their findings reveal that the respondents generally do not perceive the AQ in Hong Kong as a concern when they select this country as a tourism destination, but after their visit they considered the AQ in Hong Kong worse than in their home countries. Moreover, the results also reveal that many of the respondents were willing to pay an additional departure tax to fund improvements in AQ.
3.7.1.2 Impact on well-being and quality of life.
One set of studies ( Bohm and Pfister, 2011 ; Hipp and Ogunseitan, 2011 ; Pant et al. , 2018 ; Sato et al. , 2016 ) analyses the impact of AQ on well-being and QOL. Environmental problems experienced during the trip may affect travellers’ assessment of their QOL, as stated by Bohm and Pfister (2011) in a study based on Germans who travelled to environmentally afflicted destinations (Australia and Bangkok) and of Germans who did not travel. A study conducted in the California beaches by Hipp and Ogunseitan (2011) , using objective and subjective measures of AQ, highlights the important impact of AQ on some aspects of visitors’ QOL, through ordinal logistic models. The perceived AQ, measured using a scale from “very unhealthy” to “very healthy”, has a significant positive influence on the perception of psychological restorativeness as a whole and four dimensions of this construct – fascination, coherence, compatibility and legibility. Moreover, visitors are much more likely to perceive a higher psychological restorativeness in days considered as healthy AQ, taking into account an objective measurement of ground-level ozone concentrations. This is noticed for restorativeness as a whole and to its five dimensions considered in the study – being away, fascination, coherence, compatibility and legibility.
The impact of the exposure to air pollutants perceived by tourists and their potential health risks was also a focus in some studies such as Pant et al. (2018) and Sato et al. (2016) . The first study was carried out in Vietnam, concluding that the exposure of a tourist to air pollutants in Vietnam is lower than in cities in India and China. The second study was carried in China (Beijing) and confirmed the impact of short-term exposure to high concentrations of PM (PM 2.5 and PM 10) on tourist health, specifically on the cough reflex threshold, urge-to-cough and pulmonary function. Authors remark that a higher risk can exist in the case of unhealthy and health fragile groups (e.g. elderly, children and people with asthma or other pulmonary diseases).
3.7.1.3 Impact on visitors’ satisfaction
Only four studies ( Agarwal et al. , 2018 ; Peng and Xiao, 2018 ; Saura et al. , 2018 ; Wu et al. , 2018 ) examine the impact of AQ on visitor satisfaction. Factors influencing Chinese satisfaction with international self-drive holidays were analysed in Wu et al. (2018) . AQ is one of the factors analysed. Findings show that for the Chinese drive tourists, AQ has a positive and significant effect on their overall travel satisfaction. Moreover, Peng and Xiao (2018) also observed that in the case of domestic tourists of Beijing, the perception of experience risk produced by smog could cause travel dissatisfaction. Furthermore, Agarwal et al. (2018) examine whether hotel review scores provided by guests travelling in Singapore and Hong Kong in three online platforms – TripAdvisor.com , Agoda.com and Expedia.com – are influenced by haze episodes. Serious haze episodes showed to have a negative impact on online review scores, which reveals a decrease on guest satisfaction levels. Saura et al. (2018) analysed tweets of 25 Spanish hotels on social media, with the aim of investigating the experience of hotel guests. The authors try to identify environmental factors among comments grouped into negative and positive, according to guest feelings. Environmental factors related to atmospheric contamination emerge with considerable frequency, among negative and positive tweets. This means that these features are relevant for hotel guests and can trigger positive feelings when people perceive a good AQ. On the other hand, when contamination exists and there are risks of asthma and other breathing problems, negative feelings emerge.
3.7.1.4 Impact on destination image.
Despite that, theoretically, AQ is a relevant attribute to the competitiveness of tourism destinations, the research in this field is very scarce. Only the studies carried out by Becken et al. (2017) and Peng and Xiao (2018) investigate the impact of AQ on destination image. The model developed by Becken et al. (2017) is tested among Americans and Australians, and results reveal that feelings towards the air (affective risk perceptions) have a negative impact on both the cognitive and affective image of China. However, no significant differences are detected on feelings towards the risk of AQ between American and Australian citizens. Moreover, concerning China domestic tourists, the majority agree that smog has a negative influence on Beijing’s image, as concluded by Peng and Xiao (2018) .
3.7.2 Impact on global tourism demand.
There are also studies that address the impact of AQ on tourism but at the macro level. That is, not analysing the individual decisions of the tourist, but looking at the tourism industry of a country or region or a specific tourism attraction (such as a natural park). A consensual conclusion is that air pollution reduces the number of tourists ( Anaman and Looi, 2000 ; Deng et al. , 2017 ; Wang et al. , 2018 ; Sajjad et al. , 2014 ; Zhou et al. , 2018 ; Liu et al. , 2019 ; Keiser et al. , 2018 ; Yan et al. , 2019 ; Chen et al. , 2017 ). For instance, Anaman and Looi (2000) , using two different methodologies, estimated that 1997 and 1998 haze-related air pollution in Brunei caused about 3.75 or 28.70 per cent reduction in the number of tourists and that the total direct economic loss suffered by the tourism industry was estimated to be about B$1m to B$8m (respectively, for each methodology). Furthermore, these negative economic losses and negative impacts on tourist demand are very reliant on the phases of business cycles ( Chen et al. , 2017 ). Another example of clear evidence of negative impacts of bad AQ on tourists, as well as on human health, is the study of Keiser et al. (2018) , for the USA national parks. They found a strong negative relationship between ozone concentrations and park visitation.
The impact of AQ on tourism can vary when different pollutants are analysed. For instance, Liu et al. (2019) concluded that carbon dioxide has no significant impact on tourism while PM 2.5 has a significant negative impact. The reason for this result may be that the effect of PM 2.5 on air is that its more perceptible compared to CO 2 (colourless and odourless). Yan et al. (2019) concluded that SO 2 has the largest impact on tourism demand, followed by PM 2.5, NO 2 and PM 10, while CO (carbon monoxide) and O 3 seem to have little influence.
Another interesting result comes from Zhou et al. (2018) , who reveal that the negative impact on tourism is higher when pollution increases. For low levels of pollution, there are almost no perceived impacts, but as AQ further deteriorates, tourists become more alert to its adverse effect, and thus, the negative impact of air pollution occurs.
The impacts of AQ can also be different between domestic and international tourists ( Liu et al. ,2019 ), overnight visitors and one day visitors ( Poudyal et al. , 2013 ), as well as visitors and local residents ( Yan et al. , 2019 ). Liu et al. (2019) concluded that for China, domestic tourists are more sensitive than international tourists. The reason may be that international visitors are not able to perceive the AQ of China or have little or no information about this condition before travelling to the country. Poudyal et al. (2013) estimated elasticity for a national park in the USA, revealing that a programme aiming to improve the average visibility by 10 per cent (5.5 km) from the current level could result in an increase of about one million annual recreational visits. However, the increase would be higher for overnight visitors than for day visitors because the elasticity of tourism demand with respect to visibility was higher in overnight visitors. Yan et al. (2019) also estimated that the effect of pollutants is at least four times smaller on visitors than on local residents.
Time is also an important variable, as pollution worsens, the impact of pollution will last for a longer period and the degree of the impact in each time period will be more severe ( Zhou et al. , 2018 ). Some authors identify a delay effect in the impacts of AQ on tourism demand (five days in the case of Wang et al. (2018) and one month in the case of Zhou et al. (2018) . Poudyal et al. (2013) concluded that park visitations in a given month are significantly affected by the cumulative effect of the visibility condition in both the current and proceeding months.
Some authors have already indicated that the study of the impact of air pollution on tourism variables may be enriched with the introduction of some control variables such as tourism resource endowments, namely, the level of transport infrastructure, open-up degree, accommodation facilities ( Deng et al. , 2017 ) or disposable income level ( Wang et al. , 2018 ). Deng et al. (2017) also conclude that air pollution in nearby regions also affects local tourism, being the spillover effect (indirect effect) even larger than the direct effect.
4. Conclusions
A systematic review was performed to study the subject of impacts of AQ on tourism demand, analysing the different methods and approaches used to assess these impacts and the results obtained. A total of 26 papers were identified, with the majority published in the past decade (88 per cent) and quite restricted/focussed to China and Southeast Asia regions.
The reduced number of studies analysing the impact of AQ on tourism and the diversity of dimensions of AQ or tourism demand considered in these studies, make it difficult to draw conclusions on this kind of impact. However, some trends are observable. Both research on global tourism demand and on individual perceptions reveal that AQ tends to have a positive influence on tourism demand, with decreases in AQ leading to decreases in tourism flows or to a lower likelihood of visiting certain destinations.
The studies reviewed confirm that nobody would like to travel to those places where the environment is severely polluted. Compared with other environmental pollution such as water and soil pollution, air pollution is much more visible and can be perceived more easily by the public, which justifies the high impact that it may have on tourism in a given destination. Special attention should be devoted to avoiding high levels of pollution and bad conditions regarding AQ, as the impact of AQ on tourism tends to be higher when AQ is significantly reduced.
The results and conclusions of the present study can contribute to tourism management in similar destinations around the world. Hereby, more attention should continue to be devoted to inspecting the influences of any changes in atmospheric conditions on the demand for tourism, as extreme weather events are becoming more intense and more frequent.
Although some research studies have examined the negative impacts of air pollution on tourism, this important area of inquiry is still in its early stages and many critical issues have yet to be analysed and discussed. The most notable issues are how AQ influences the seasonality of tourism demand, tourism experience, attractiveness and competitiveness of tourism industry; and how it influences the magnitude and nature of the economic impacts of tourism industry. There is further lack of studies, which relate AQ impacts to population exposure (pollutant concentration multiplied by people and time). Therefore, more secondary data related to regional and national impacts of tourism activities has to be included into the analysis of the relationship between AQ and tourism. As previously mentioned, China and Asiatic countries have been extensively analysed under this issue. However, little is known about other regions and nations around the world where AQ levels are low or are significantly affected by high levels of air pollution.
Besides that, there is still a limited number of studies examining the role of AQ in the attractiveness and competitiveness of tourism destinations, and the question about the effects of AQ over tourism destination choices remains unanswered. Then, very little concern is devoted to good AQ and how the AQ index can become an important destination attribute influencing the attractiveness of tourism destinations.
Despite being a systematic literature review, this study has limitations that need to be addressed. The first is that the studies analysed, i.e. those focussed on the effects of outdoor AQ on tourism, are very scarce. This partially results from the option to only include studies focussed on outdoor AQ. As AQ is extremely linked to physical comfort and may have impacts on the tourist experience, future research should include studies on indoor AQ, providing the opportunity to strengthen the sample and to establish some comparisons between two different, but in a certain way, related matters.
Another limitation is the fact that most of the studies were focussed on Asian countries, with very few being conducted in other regions of the world. Although being an uncontrolled issue, there is an opportunity for future studies to be developed, helping to understand if the findings obtained in Asian countries are aligned and coherent with other regions, namely, in a context where environmental awareness is a growing phenomenon.
Finally, the option to only include papers in English can also be pointed out as a limitation, namely, because they may not be representative of all the evidence on the topic in analysis. Therefore, future research should be extended to included literature published in other languages.
Considering the great need of carrying out more studies, especially in other regions of the world beyond Asian countries, to ensure a sustainable development of tourism in the future, a wide plethora of methodological approaches may be adopted. As already mentioned, secondary data should be further explored. Moreover, mixed methodological approaches, including both quantitative and qualitative methods, should be privileged in further research to obtain a deeper knowledge of how AQ affects tourism demand and, consequently, the competitiveness of tourism destinations. Considering the environmental changes that have been occurring and that will take place in the future, longitudinal studies are also highly relevant to assess how the impact of AQ on tourism demand is changing and what kind of strategies should be designed to ensure sustainable development. The ongoing Portuguese research project ARTUR ( http://projeto-artur.web.ua.pt ) will address some of these concerns and its outcomes may help to increase the knowledge on both the environmental and tourism sectors, promoting both AQ protection and tourism sustainability.
Acknowledgements
Thanks are due for the financial support to FCT/MCTES through national funds, and the co-funding by the FEDER, within the PT2020 Partnership Agreement and Compete 2020, for the ARTUR project (POCI-01-0145-FEDER-029374) and CESAM (UID/AMB/50017 – POCI- 01-0145-FEDER-007638).
PRISMA flow diagram of the article selection process
Number of papers published by year of publication
Geographical location of the study areas focussed and covered by the reference
Word frequency represented by word clouds according to abstracts, titles and keywords
Information on the publication, authorship and citations (continues)
| Authors (year of publication) | Title of the paper | Journal or proceedings | Domain of the journal or proceedings | Citations in SCOPUS | Citations in Google Scholar |
|---|---|---|---|---|---|
| Economic impact of haze-related air pollution on the tourism industry in Brunei Darussalam | Economics, econometrics and finance: economics and econometrics | 14 | 31 | ||
| (2000) | Visitor Perceptions and Valuation of Visibility in the Great Gulf Wilderness, New Hampshire | a) | a) | 8 | |
| Air Quality in Hong Kong: A Study of the Perception of International Visitors | Business, management and accounting: tourism, leisure and hospitality management | 13 | 21 | ||
| Tourism in the Face of Environmental Risks: Sunbathing under the Ozone Hole, and Strolling through Polluted Air | Business, management and accounting: tourism, leisure and hospitality management | 1 | 4 | ||
| Effect of environmental conditions on perceived psychological restorativeness of coastal parks | Psychology: applied Psychology | 30 | 53 | ||
| (2013) | Estimating the impact of impaired visibility on the demand for visits to national parks | Business, management and accounting: tourism, leisure and hospitality management | 13 | 18 | |
| (2014) | Climate change and air pollution jointly creating nightmare for tourism industry | Environmental science: pollution | 25 | 39 | |
| (2015) | The Influence of Perceived Environmental Impacts of Tourism on the Perceived Importance of Sustainable Tourism | Business, management and accounting: tourism, leisure and hospitality management | 4 | 6 | |
| (2015) | Tourists’ Perception of Haze Pollution and the Potential Impacts on Travel: Reshaping the Features of Tourism Seasonality in Beijing, China | Social sciences: geography, planning and development | 28 | 40 | |
| (2016) | Effect of Short-Term Exposure to High Particulate Levels on Cough Reflex Sensitivity in Healthy Tourists: A Pilot Study | Medicine: Pulmonary and Respiratory Medicine | 2 | 4 | |
| (2017) | Urban air pollution in China: destination image and risk perceptions | Business, management and accounting: tourism, leisure and hospitality management | 11 | 20 | |
| (2017) | Evaluating impact of air pollution on China’s inbound tourism industry: a spatial econometric approach | Business, management and accounting: tourism, leisure and hospitality management | 4 | 6 | |
| (2018) | Blessing in disguise? Environmental shocks and performance enhancement | ||||
| Research on the Tourists’ Type and Behavior based on the Fog and Haze Perception: Taking Xi’an as a Case | Environmental science: general environmental science | 0 | 0 | ||
| (2018) | Air pollution and visitation at US national parks | Multidisciplinary | 3 | 4 | |
| (2018) | Exposure to air pollutants in Vietnam: Assessing potential risk for tourists | Environmental Science: general environmental science | 1 | 2 | |
| How does smog influence domestic tourism in China? A case study of Beijing | Business, management and accounting: tourism, leisure and hospitality management | 1 | 1 | ||
| (2018) | Attitudes Expressed in Online Comments about Environmental Factors in the Tourism Sector: An Exploratory Study | Environmental science: health, toxicology and mutagenesis | 10 | 4 | |
| (2018) | Effect of air quality in the place of origin on outbound tourism demand: Disposable income as a moderator | Business, management and accounting: tourism, leisure and hospitality management | 3 | 4 | |
| (2018) | Chinese behind the wheel: factors affecting their satisfaction with international self-drive holidays | Business, management and accounting: marketing | 0 | 0 | |
| (2018) | Air quality and the visitor experience in parks and protected areas | Business, management and accounting: tourism, leisure and hospitality management | 2 | 2 | |
| (2018) | Air quality and inbound tourism in China | Business, management and accounting: tourism, leisure and hospitality management | 1 | 2 | |
| Analysis on the Impact of haze on Beijing Residents' Traveling Intention and Decision-Making | Engineering: general engineering | 0 | 0 | ||
| (2019) | Tourism Development, Environment and Policies: Differences between Domestic and International Tourists | Social sciences: geography, planning and development | 0 | 0 | |
| (2019) | Exploring the effect of air pollution on social activity in China using geotagged social media check-in data | Social sciences: urban studies | 1 | 0 |

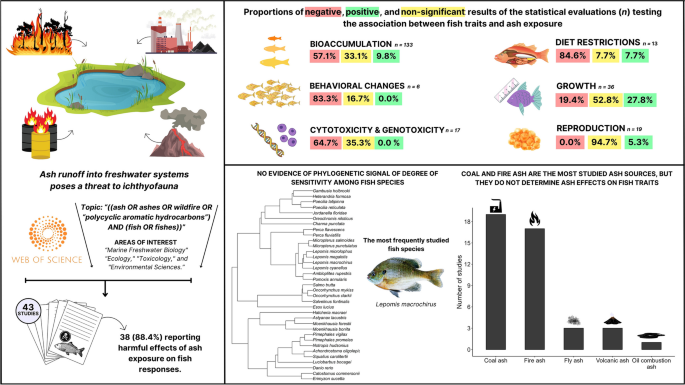
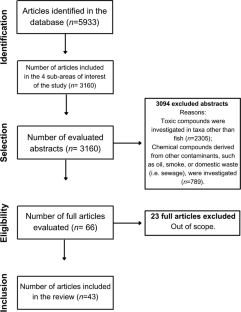



IMAGES
VIDEO
COMMENTS
This review (178 published articles) is the first to systematically examine the psychological (affective, cognitive, behavioral), economic, and social effects of air pollution beyond its physiological and environmental effects. Affectively, air pollution decreases happiness and life satisfaction, and increases annoyance, anxiety, mental disorders, self-harm, and suicide.
A systematic literature review and critical appraisal of epidemiological studies on outdoor air pollution and tuberculosis outcomes. Environ. Res. 170 , 33-45 (2019).
The current work provides the most systematic assessment of the current literature on ambient air pollution and health. Multi-pollutant preventive approaches are required to enhance the comprehensiveness of the impacts of air pollution on human health. ... A systematic review of air pollution and incidence of out-of-hospital cardiac arrest. J ...
Objective: To analyze the state of the art on the effects of air pollution on human health through a mapping review of existing systematic reviews and meta-analyses (SRs and MAs). Methods: The systematic mapping review was based on the recommendations for this type of scientific approach in environmental sciences. The search was performed using ...
Indoor air pollution from unprocessed solid fuel use and pneumonia risk in children aged under five years: a systematic review and meta-analysis. Bull World Health Organ . (2008) 86 :390-4. 10.2471/BLT.07.044529 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
Air pollution, currently on several global health agendas, has rapidly become a global problem with the increasing global urbanisation, transportation-related emissions, and increased energy consumption. ... This was a systematic literature review and meta-analysis of articles published in English from January 1st, 1946, through May 31st, 2022 ...
This systematic review assessed to evaluate the potential correlation between oral health and air pollution. To the best of the authors' knowledge, this is the first systematic review endeavoring to compare air pollution and oral health. A systematic search was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) statement and employed the ...
Ambient air pollution is the leading environmental risk factor for disease globally. Air pollutants can increase the risk of some respiratory infections, but their effects on tuberculosis (TB) are unclear. In this systematic literature review, we aimed to assess epidemiological studies on the associ …
The objective of this umbrella review was to investigate comprehensive and synthesized evidence of the association between ambient air pollution and obesity based on the current systematic reviews and meta-analyses. Related studies from databases including PubMed, EMBASE, Web of Science, and the Cochrane Library, published before July 16, 2023, were considered in the analysis.
The adverse health effects of exposure to air pollutants, notably to particulate matter (PM), are well-known, as well as the association with measured or estimated concentration levels. The role of perception can be relevant in exploring effects and pollution control actions. The purpose of this study was to explore studies that analyse people's perception, together with the measurement of ...
Abstract. A wide range of policies, strategies, and interventions have been implemented to improve air quality all over the world. This systematic review comprehensively appraises the policies and strategies on air pollutants controls enacted in different countries, worldwide. Three databases, Web of Science, PubMed and Scopus, were used for ...
Search strategy. The present systematic review was performed according to standard methods the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) [].A comprehensive screening approach to find the urban air pollution control strategies and policies published in peer-reviewed journal was performed up to 19 January 2021 in three scientific databases: PubMed, Web of Science ...
The aim of this study is to provide an updated systematic literature review of peer-reviewed epidemiological studies that examined the health impacts of outdoor air pollution in Australia, including short- and long-term exposure. Following PRISMA guidelines, we conducted a systematic literature review. Broad search terms were applied to two ...
A systematic literature review and critical appraisal of epidemiological studies on outdoor air pollution and tuberculosis outcomes. ... Childhood tuberculosis and exposure to indoor air pollution: a systematic review and meta-analysis. Int. J. Tuberc. Lung Dis, 19 (5) (2015), pp. 596-602, 10.5588/ijtld.14.0686.
Background Air-pollution and weather exposure beyond certain thresholds have serious effects on public health. Yet, there is lack of information on wider aspects including the role of some effect modifiers and the interaction between air-pollution and weather. This article aims at a comprehensive review and narrative summary of literature on the association of air-pollution and weather with ...
Our systematic literature review of 234 articles in Scopus, WOS, and PubMed databases returned 51 relevant research articles. Findings show that particular environments have detrimental effects on outdoor air quality, which in turn have a negative impact on childhood asthma.
We conducted a systematic literature review on the application of data mining and machine learning methods in air pollution epidemiology. We carried out our search process in PubMed, the MEDLINE database and Google Scholar. Research articles applying data mining and machine learning methods to air pollution epidemiology were queried and reviewed.
There is an urgent need by the European Union to establish baseline levels for many widespread pollutants and to set out specific levels for these under the Zero pollution action plan. To date, few systematic reviews, superseded by bibliometric analyses, have explored this issue. Even less research has been carried out to compare the efficacy of these two data extraction approaches. This study ...
Whether air pollution affects female infertility is under debate. The aim of the present study was to conduct a systematic review of studies that evaluated the impact of air pollution on female infertility. We systematically searched the MEDLINE (PubMed) and SCOPUS databases to identify all relevant studies published before October 2017.
This systematic review (Lam et al., 2016) was the first systematic review and metaanalysis of the literature on the association between autism spectrum disorder (ASD) and air pollution and ultimately concluded that there was "limited evidence of toxicity." While there was a relatively rich database of human evidence, we found several ...
The objective of this paper is to review what is known and has been published, about the impact of outdoor AQ on tourism demand, using a systematic literature review method. To date, there is no literature review study on this topic. It is of note that the impact of tourism on AQ was also not addressed.
We conducted this comprehensive review to explore the association between ambient air pollution and sleep quality. A systematic search was conducted with the databases of PubMed and Web of Science from inception to November 2019. Overall, 15 studies with 133,695 subjects that evaluated the association between ambient air pollution and sleep ...
The health effects of traffic-related air pollution continues to be of public health interest, with highest exposures in urban settings and residences in proximity to busy roadways. Following its well-cited 2010 critical review, in early 2018 the HEI Board of Directors appointed an expert HEI panel to review the traffic and health literature.
Ash runoff into freshwater systems from fire events, coal combustion, and volcanic activities threatens to biodiversity conservation, given its toxicity to various aquatic organisms. However, despite many studies reporting a negative relationship between ash exposure and the biological traits of freshwater fish, non-significant and even positive associations can also be found in the literature ...
Microplastic fibre (MPF) pollution is a pressing concern that demands urgent attention. These tiny synthetic textile fibres can be found in various ecosystems, including water and air, and pose significant environmental risks. Despite their size (less than 5 mm), they can harm aquatic and terrestrial organisms and human health. Studies have demonstrated that these imperceptible pollutants can ...
7. Conclusions. This systematic review comprehensively reviews the studies on various factors that affect air pollution exposure during travel and the influence of air pollution exposure on travel behaviour. It was found that the type of travel mode plays a vital role in travellers' daily exposure to air pollution.
Background There is a consistent association between exposure to air pollution and elevated rates of cardiopulmonary illnesses. As public health activities emphasize the paramount need to reduce exposure, it is crucial to examine strategies like the antioxidant diet that could potentially protect individuals who are unavoidably exposed. Methods A systematic search was performed in PubMed ...
A systematic review of air pollution as a risk factor for cardiovascular disease in South Asia: limited evidence from India and Pakistan Int J Hyg Environ Health. 2014 Mar ... A literature search was conducted in PubMed and Web of Science. Our inclusion criteria included peer-reviewed, original, empirical articles published in English between ...
The aim of this paper is to provide, through a systematic literature review, an overall picture of the relationships between air pollution and cognitive outcomes in children and adults, and to identify areas for future research. ... Global association of air pollution and heart failure: a systematic review and meta-analysis. Lancet, 382 (2013 ...
Editors' Note: Short-Term Exposure to Air Pollution and Ischemic Stroke: A Systematic Review and Meta-Analysis ... A Systematic Review and Meta-Analysis. Editors' Note: Short-Term Exposure to Air Pollution and Ischemic Stroke: A Systematic Review and Meta-Analysis Neurology. 2024 Aug 13;103(3):e209633. doi: 10.1212/WNL.0000000000209633. Epub ...