- High contrast
- Press Centre

Search UNICEF
Keynote speech to the world health summit 2021 – 24 october 2021, unicef executive director henrietta fore.
Excellencies, colleagues, friends … it is a pleasure to be with you here today for the World Health Summit.
I am honoured and inspired by the spirit of collaboration among experts in science, politics, business, government and civil society represented at this Summit.
On behalf of UNICEF, I am grateful for the opportunity to speak with you now at this critical moment in the global response to the COVID-19 pandemic – a pandemic which continues to impact so many aspects of our lives. COVID-19 has hobbled economies, strained societies and undermined the prospects of the next generation. While children are not at greatest direct risk from the virus itself, they continue to suffer disproportionately from its socioeconomic consequences. Almost two years into the pandemic, a generation of children are enduring prolonged school closures and ongoing disruptions to health, protection and education services.
That is why today I am here to discuss the health threats facing the 2.2 billion children around the world who UNICEF serves, and the opportunity we have to protect them.
Driven by new variants of concern, the virus continues to spread. While successful vaccination campaigns in the wealthy world have driven down rates of hospitalization and death, millions in low income countries await their first dose, and fragile health systems – on which children rely – are in jeopardy.
Yet the gap between those who have been offered vaccination against COVID-19 and those who have not is widening. While some countries have protected most of their populations, in others, less than 3 per cent of the population have had their first dose. Those going without vaccines include doctors, midwives, nurses, community health workers, teachers and social workers – the very people that children, mothers and families rely upon for the most essential services.
This is unacceptable. As a community of global health leaders, we have a choice. We can choose to act to reach more people with vaccines. This will keep people safe AND help to sustain critical services and systems for children.
Today, almost 7 billion doses of COVID-19 vaccine have been administered, less than a year since the first vaccine was approved. And we are now on track to produce enough vaccines to protect the majority of people around the world before the end of next year.
But will we protect everyone?
Will we send lifesaving, health-system-saving COVID-19 vaccines to the world’s doctors, nurses, and most at-risk populations?
Will donors continue to fund ACT-A and COVAX sufficiently to procure and successfully deploy the tests, treatments and vaccines needed to end the pandemic? Or will the costs of in-country delivery fall on struggling economies so that they are forced to cut other lifesaving health programmes such as routine childhood vaccinations?
Will we stand by as the lowest-income countries, with the most fragile health systems, carry on unprotected – risking high death rates due to shortages of tests, treatments and vaccines? Or will we invest so that community health systems everywhere can withstand further waves of the virus, and bounce back from future shocks?
Will we allow new variants of the virus to flourish in countries with low vaccination rates? Or, will we reap the benefits of global cooperation to defeat this global problem, together?
The world has learned that financing for prevention, preparedness and response is insufficient and not adequately coordinated. And that is a vital lesson.
But even more fundamentally, we have learned that the underlying strength of the health sector in general is a critical factor in a country’s ability to weather a storm like COVID-19.
After all, what good are vaccines if there is no functioning public health system to deliver them?
How do we hope to contain outbreaks if there are not enough trained and paid healthcare workers?
This pandemic has been crippling for high income countries where average spending on healthcare per capita exceeds $5,000. So, it is hardly surprising that it is causing critical strain in lower-income countries where the average per capita expenditure on healthcare each year is less than $100.
The past 22 months have shown us that even as we battle immediate threats such as a pandemic, we must also ensure continuous access to essential health services. If we do not, there will be an indirect increase in morbidity and mortality.
As COVID-19 took hold of the world, healthcare workers serving pregnant mothers, babies and children faced unthinkable choices. As COVID patients gasped for breath, desperate for oxygen, mothers and babies needed it too. As wards filled up with virus victims, staff were not free to help the very young. As health budgets were stretched to the breaking point, routine healthcare began to go by the wayside.
These are some of the reasons why more than twice as many women and children have lost their lives for every COVID-19 death in many low and middle-income countries. Estimates from the Lancet suggest up to nearly 114,000 additional women and children died during this period.
I greatly fear that the pandemic’s impact on children’s health is only starting to be seen.
While the pandemic has underscored that vaccination is one of the most cost-effective public health interventions, we have already seen backsliding in routine immunization. In 2020, over 23 million children missed out on essential vaccines – an increase of nearly 4 million from 2019, with decades of progress tragically eroded.
Of these 23 million, 17 million of them did not receive any vaccines at all. These are the so-called zero-dose children, most of whom live in communities with multiple deprivations.
Here are some of the most urgent choices we could make to address these problems:
Governments can share COVID-19 doses with COVAX as a matter of absolute urgency and resist the temptation to stockpile supplies more than necessary.
Governments can also honour their commitments to equitable access and make space for COVAX and other parts of ACT-A at the front of the supply queue for tests, treatments, and vaccines as they roll off production lines.
Manufacturers can be more transparent about their production schedules and make greater efforts to facilitate and accelerate equitable access to products. This will help to ensure that COVAX and ACT-A get supplies faster.
Governments, development banks, business and philanthropy can target strategic, sustainable investments in building robust and resilient primary healthcare services – embedded in each and every community.
We can and we must choose a path ahead that is equitable, sustainable and rooted in the principle that every human being, young and old, rich and poor, has the right to good health.
And there is good reason to believe that now is the time to set ourselves upon that path.
A look back at history shows us that global threats and crises that challenge multiple interests and equities have a way of pulling together diverse partners to solve shared problems. Indeed, it is out of some of the most tragic crises that the world has found some of the best solutions.
I believe now is such a time. We have a historic opportunity to both end the COVID-19 pandemic and set out on the road towards eradicating preventable diseases, ending avoidable maternal, newborn and child deaths, and building a strong foundation for community health that will serve this generation and the next.
We can and we must seize this moment together.
Thank you.
Media contacts
About unicef.
UNICEF works in some of the world’s toughest places, to reach the world’s most disadvantaged children. Across more than 190 countries and territories, we work for every child, everywhere, to build a better world for everyone.
Follow UNICEF on Twitter , Facebook , Instagram and YouTube
Related topics
More to explore, reaching children who missed out on vaccines in brazil.
Discover how community health workers navigate rural rivers and bustling cities to reach those who need vaccines most
Kingdom of Saudi Arabia pledges US $500 million to protect children around the world from polio and end the disease for good
UNICEF commends Bhutan for vaccinating almost all children with life-saving vaccines in historic feat
WHO and France convene high-level meeting to defeat meningitis
publication
Short Messages Encouraging Compliance with COVID-19 Public Health Guidelines Have Minimal Persuasive Effects
Sophia Pink, Michael Stagnaro, James Chu, Joe Mernyk, Jan Voelkel, Robb Willer
Preventing the spread of COVID-19 requires persuading the vast majority of the public to significantly change their behavior in numerous, costly ways. Many efforts to encourage behavior change – public service announcements, social media posts, speeches, billboards – involve relatively short, persuasive messages. Here, we report results of five experimental tests (N = 5,351) of persuasive short messages conducted in the US from March – July 2020. In our first two studies participants rated the persuasiveness of 56 unique messages (31 drawn from the social science literature, 25 crowdsourced from online respondents). We then conducted three well-powered, pre-registered experiments testing whether the four top-rated messages would increase intentions to comply with public health guidelines. We compare messages to both a null control condition and an “active control” message that included a reminder of the virus and suggested behaviors with no persuasive frame. Five messages in the initial studies were rated as more persuasive than a control, and four messages in the later studies increased behavioral compliance intentions relative to a null control. However, none of these messages had consistent effects when compared to the active control message. We conclude that it may not be practically possible to identify short messages that reliably out-perform a simple reminder of the virus and recommended behaviors during the advanced stages of the pandemic. The most persuasive message studied was one emphasizing people’s civic responsibility to reciprocate healthcare workers’ sacrifices, which performed best in three of five studies.
How Is America Still This Bad at Talking About the Pandemic?
America’s leaders could stand to learn four lessons on how to communicate about COVID.

With cases decreasing, well more than 65 percent of the eligible population inoculated with effective vaccines, and new COVID therapeutics coming to market, the United States is in very different circumstances than it was in early 2020. Life is currently feeling a little more stable, the future a good deal more clear.
But one thing about the pandemic has remained largely unchanged: Political and scientific leaders are still struggling to communicate recommendations to the American public. Are mask mandates warranted at work and school? First we were told no; then, yes; now the answer, for good reasons this time, is changing again. Are fourth mRNA shots necessary for the most vulnerable? First the CDC said no; then, to get one five months after the third dose; and now the waiting period has been reduced to three months.
The Omicron surge that the country is now exiting may not be our last of this pandemic, and SARS-CoV-2 will surely not be the last virus to cause a pandemic . If we are to get through whatever lies ahead without more unnecessary mass death, we need to reflect on how pandemic communication has fallen short and how the country can get better at it. Over the past six months, I have planned and led a small faculty seminar at the Harvard T. H. Chan School of Public Health on the pandemic, the press, and public policy. I’ve gleaned four lessons about transmitting clear, practical information in changing circumstances. Our leaders would be wise to heed them.
1. The conventional wisdom about avoiding ambiguity and uncertainty is wrong.
A former local public-health official told me last year that aides to the elected official for whom they worked had advised them that the key to pandemic communications was to “keep it simple; never say ‘on the other hand.’” This may (or may not) be good practice in an election campaign, but it has proved both common and exceedingly bad counsel in a pandemic, when officials frequently need to offer guidance from a position of uncertainty.
In March 2020, for example, public-health officials needed to tell people whether they should avoid contact with suspect surfaces and whether they needed to wear masks outside clinical settings. In an excess of caution and based on experience with other pathogens, the CDC advised Americans to wipe things down. But when it came to masks, the agency seemed to abandon that precautionary approach. The situation was complicated: The best masks were in terribly short supply and urgently needed by the health-care system. Rather than receiving an explanation of the situation and advice to improvise cloth masks, the public was told to forgo masks altogether because they were unnecessary.
Read: How to talk about the coronavirus
Public-health officials’ failure to trust Americans with the truth was not sophisticated or even practical. When the advice was belatedly revised in a manner that revealed it had always been faulty, an erosion of trust began and has only accelerated over the ensuing two years.
Moreover, this mistake has been repeated again and again in new contexts. Last summer, for instance, advice was given to take off your mask outside, only to be sort of retracted for fear that people would not wear them in crowds, or inside, especially as Delta struck. Throughout the past year, there has been far too much reluctance to offer varying advice to the vaccinated and unvaccinated, and to the very young and very old.
Officials (and the press responsible for critiquing and distilling their advice) need to be more candid about uncertainty, more open about asking people to mitigate risks temporarily until our knowledge increases, more willing to vary guidance for different groups without worrying that this constitutes “mixed messaging.” In the short run, such an approach may be challenged as weakness, but in the long run it will be revealed as building credibility, trust, and thus strength.
2. In a pervasive crisis, science must adjust to politics.
Over and over in the pandemic, public-health officials have been both surprised and disappointed to find out that concerns they consider “political” have trumped scientific knowledge. Not only their surprise but even a measure of their disappointment is worth reconsidering.
This is not to say that public health should be held hostage to conspiracy theories or sheer mendacity, as was sometimes the case in the first year of the pandemic, when President Donald Trump was promoting quack cures and stubbornly resisting masking. But if “Follow the science” was once a watchword of public-health resistance, it later came to sometimes embody naivete. In a well-functioning system, science is not oppositional to politics, but neither does it supersede politics . Both are essential in a democratic society; they must coexist.
Jay Varma: Not every question has a scientific answer
When a public-health concern becomes a pervasive national crisis, under any leadership, it is inevitable—and actually proper—that what may be narrowly in the interest of optimal medical outcomes will be weighed against impacts on the economy, equity, educational imperatives, national security, and even national morale. In our democratic system, that weighing is left to our elected officials. Those officials have a duty to arm themselves with the best public-health advice, and public-health experts are obligated to make sure that both leaders and the public have access to that advice, whether the politicians wish to know it or not.
In retrospect, the United States might have been wise to impose fewer restrictions on elementary and secondary schools over the past two academic years—not because school closures didn’t help stop the spread of the virus, but because the educational and economic losses from widespread remote schooling might have outweighed the gains in reduced cases. The question is clearly more than scientific.
Top officeholders and scientists alike can do a better job of accommodating each other. On the one hand, political leaders would do well to remember that many of the most senior officials in relevant agencies, even those with appropriate professional training, have likely been selected (by them!) for political reasons, and may or may not be the most expert in a particular situation. It can be a grave error, particularly in a place like the White House, to make the leap from “We have our own doctors” to “We have the best doctors.”
Matthew Algeo: Presidential physicians don’t always tell the public the full story
On the other hand, scientists (and even amateur epidemiologists) would do well to formulate their advice to political executives with empathy for their perspective. This does not mean shading the truth or telling someone what you think they want to hear, but it does mean safeguarding a leader’s credibility and acknowledging the political or practical constraints they face. It also means understanding that, once decisions are made, as President John F. Kennedy reportedly observed, leaders must live with them while advisers can move on to other advice. President Joe Biden, for instance, has too often found himself personally announcing conclusions that were not yet certain and guidance that was likely to soon change.
3. Speak the same language the public does.
Communication is difficult when people are not speaking the same language . In the pandemic, we have seen this play out in two major ways. First: Scientists use words they think their listeners understand, only to find out much later that they don’t. Some researchers concluded early on that SARS-CoV-2 was what they term “airborne.” When many people responded by limiting the big change in their behavior to standing six feet apart, the scientists were enormously frustrated. That’s because by “airborne,” they didn’t mean merely that the virus was borne through air, but that it was aerosolized, and thus highly contagious, especially indoors . They wanted the public to stop interacting closely, especially indoors and unmasked. Recognizing earlier that the scientific and colloquial understandings of airborne didn’t match in this context would have made a difference, at least in messaging and possibly in consequences.
Read: Nine pandemic words that almost no one gets right
Second: Only a distinct minority of the population has a firm grasp of statistics, but many scientists communicate as if everyone does. In addition to emphasizing the rarity of vaccine side effects or the significant protection offered by the shots, officials must give the public a lens through which to understand the exceptions some of them are sure to encounter in their daily lives.
If a particular finding, for instance, applies to 99 percent of Americans, scientists and public officials need to acknowledge—clearly, candidly, right up front—that more than 3 million people will have a different experience from that norm. To duck this reality is to risk the sheer number of counterexamples seeming to “disprove” the valid conclusion. This is especially important in communicating to and through the press.
4. Never forget the heroes.
The darkest early days of the pandemic were redeemed somewhat by the national rallying around health-care professionals, first responders, and other essential workers. That focus on the heroes among us underlined the fact that, in a pandemic, we are fundamentally in the fight together, and the virus is our common enemy.
Leaders made a crucial communications mistake in not extending this lesson to the rollout of the vaccines, which were the result of both the genius and the hard and astoundingly fast work of another set of heroes. Greater celebration, beginning in late 2020, of these innovators, inventors, and even manufacturers could, I think, have made widespread division over the vaccines less likely and less pervasive.
From the January/February 2021 issue: How science beat the virus
It would, for instance, have helped if the editors of Time magazine had felt compelled to name the inventors of the mRNA vaccines as the 2021 “People of the Year,” rather than deeming them runners-up to Elon Musk. Glorifying pharmaceutical companies may be a stretch, but why not loudly praise the workers who churned out the “Warp Speed” vaccines as modern-day Rosie the Riveters?
In the absence of these sorts of celebrations, the division over vaccines remains the greatest failure of the U.S. experience of the pandemic. More than a quarter of a million deaths were likely directly preventable by available vaccination. Undervaccination contributed to the horrible strength of the Delta and Omicron waves, lingering economic pain, and remote schooling, which might also have been avoided. Next time, the communication breakdown may or may not center on vaccines. But we’d all be much better off if we didn’t have a breakdown at all.
- Skip to main content
- Skip to FDA Search
- Skip to in this section menu
- Skip to footer links

The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
U.S. Food and Drug Administration
- Search
- Menu
- News & Events
- Speeches by FDA Officials
- The Critical Role of Health Care Professionals During the COVID-19 Pandemic - 08/10/2020
Speech | Virtual
Event Title The Critical Role of Health Care Professionals During the COVID-19 Pandemic August 10, 2020
(Remarks as prepared for delivery)
I’m pleased to have the opportunity today to speak with you about COVID-19, the FDA’s role in responding to this public health emergency, and the continuing challenges the agency and the medical profession face as it continues to evolve.
I’d like to begin by thanking Dr. Susan Bailey and the American Medical Association for hosting and moderating this event today, as well as the Reagan Udall Foundation for their continuing support of the FDA.
And I’d like to thank all of the physicians and health care professionals on this call today for your hard work, thoughtfulness, and commitment during this challenging time. Among the heroes who have emerged from this crisis are the health care professionals who have risked their own health to serve their patients. The nation is indebted to you.
As we move forward, we know that the pandemic continues to evolve and the health care community must continue to deliver high-quality care to all patients.
Fortunately, we’ve made significant progress in our understanding of this disease, our ability to combat it, and our efforts to help patients suffering with it.
As health care professionals and scientists, we understand there are no easy answers. We still have much more to learn about this disease, with many unanswered questions. And we need to not only treat patients with the disease, but also to prevent the spread of the disease as we seek effective therapeutics and safe and effective vaccines.
Today, I want to talk to you about some of these challenges and about the nature and importance of science and data as we search for answers.
I also want to speak with you in your role as doctors and other health professionals, who are dealing with very practical questions involving patients – an experience I understand and empathize with from my own practice as an oncologist.
Most importantly, I want to reassure you that the decisions that FDA will have to make in the coming months, with regard to new tests for COVID-19, new therapeutics, and new vaccines, will be based on good science and sound data.
Because of the speed with which we need to make decisions, there has been discussion about whether FDA will compromise any of our scientific principles in reviewing data and making decisions about new products. Let me assure you that we will not cut corners.
All of our decisions will continue to be based on good science and the same careful, deliberative processes which we have always used when reviewing medical products.
It is important that you as medical practitioners not only understand this commitment, but also that you reassure your patients.
We have seen surveys reporting that significant percentages of the public would be reluctant to take a vaccine once available. We hope that you will urge your patients to take an approved vaccine so that we can seek to establish widespread immunity.
We can emerge from this emergency only by working together.
We know that the overwhelming quantities of COVID-19 information and data that seem continually to be expanding can place a significant burden on you as clinicians seeking to respond to patient questions and, when appropriate, modify treatment recommendations.
Indeed, COVID-19 is affecting the practice of medicine in many ways, and the FDA has an important role to play in supporting providers and patients through this evolution. Although it seems as if we’ve been engaged in the battle against COVID-19 for a very long time, in the broader context of disease and science, it’s actually been a relatively short period.
Consider that as recently as this January – just eight months ago – few people, other than a limited group of health care professionals and infectious disease experts, had even heard of the novel coronavirus.
It’s easy for me to recall just how recently SARS-CoV-2 appeared on our national radar. That’s because the first reports of the outbreak began just a few weeks after I was sworn in as FDA commissioner. I’d like to share with you my own experiences and what I have learned in the past six months.
From the very beginning, this has been a perplexing and challenging medical mystery, presenting far more questions than answers. Even for those who have followed this public health crisis from its earliest days, little information or understanding of the disease was available.
We didn’t know, for instance, basic things, such as how aggressive, virulent, or contagious the virus was.
That’s not a comfortable position for health professionals who like to be well informed, particularly when we work at agencies charged with protecting the American public.
I learned quickly that despite the relative lack of knowledge, we at the FDA had to make decisions about relative benefits and risks with the data we had.
The FDA regulates the safety, effectiveness and quality of all medical products – drugs, vaccines, and medical devices. We also regulate food safety, which of course also is critical during a crisis like this.
There is always a steep learning curve in the response to a public health emergency, particularly when it involves a new disease. But this learning curve has been especially steep for all of us.
I am trained, as many of you are, as a scientist. And when this pandemic emerged, I conveyed to the leadership and staff at the FDA that even in the face of the public response to this emergency, we at the FDA needed to apply scientific rigor to any decisions being made, no matter how quickly they needed to be made,
It was reassuring to me that the FDA leadership and staff agreed whole-heartedly with this approach. This is how the FDA has always functioned in its role as a federal agency that makes regulatory decisions based on scientific rigor.
We at the FDA, and you as health care professionals have had to respond to challenges like these in real time.
For this pandemic, in particular, for the FDA this has meant supporting the development of safe and effective medical countermeasures.
These actions also included ensuring that our front-line health care workers had and will continue to have the necessary protective equipment.
Since the beginning of this pandemic, FDA scientists have been immersed in providing essential regulatory advice, guidance, and technical assistance needed to advance the development of tests, therapies, and vaccines.
And it’s meant that we have been vigilant in seeking to prevent the sale of fraudulent products that could harm the public.
To be successful in each of these efforts, we’ve been working hard to strengthen the scientific response. We’ve done this by supporting collaborative efforts, creating open communication channels, and building public-private partnerships.
For example, the FDA has created resources like reference-grade sequence data for SARS-CoV-2 to support research and reference panels for COVID-19 diagnostic tests to support continued developments in testing.
The agency has supported the National Institutes of Health’s public-private partnership for therapeutic and vaccine development.
The FDA has also partnered with a number of external partners to gather real world evidence to help inform our understanding of the natural history of COVID-19, drug utilization and performance of COVID-19 diagnostics and therapeutics.
I’m pleased that so many of you -- and the professional organizations you are part of -- have been involved in some of these collaborative efforts.
It’s essential that we bring forward the best ideas and innovations to support the development of new and effective treatments. Working together has been an instrumental part in our ability to come so far, so fast.
Our approach is consistent with and, indeed, goes to the core of the FDA’s mission; we constantly gather new information and evidence about the disease to inform our actions.
As we learn, we discover more answers. But that, in and of itself, is not enough. We must continue to be vigilant and aggressive, constantly reviewing and evaluating the data as they emerge.
The principle underlying this -- that our decisions must not only be informed by the most rigorous data and best science, but also that the evidence on which we base our continuing review is regularly refreshed and expanded through new experiences and opportunities -- is a basic approach of science.
It’s certainly a personal principle that has been a priority for me throughout my career as a physician and researcher.
We are learning more every day. For example, as doctors have treated more cases of COVID, it has become clear that it is not just a respiratory ailment but can affect many organ systems, including the kidneys and heart, and can also cause vascular complications.
And although initially, many of us believed children were not significantly affected by the COVID-19 virus, subsequent reports from across the United States and Europe showed that some young COVID patients were found to have Pediatric Multisystem Inflammatory Syndrome or PMIS.
These cases exhibited clinical features similar to Kawasaki Disease, a rare inflammatory disease primarily affecting young children, which causes blood vessels to become inflamed or swollen throughout the body.
Similarly, some dermatologists revealed that some of their patients who were later diagnosed with COVID-19 had symptoms that could be due to vasculitis, including frostbite like pain, small itchy eczema-like lesions on their extremities. and reddened patches of skin.
We are all concerned about the reports of rising case counts in different locations across the U.S., particularly in the Sunbelt states.
We have also learned that common sense public health measures such as the wearing of masks, social distancing, hand-washing, protection of the vulnerable, and avoidance of large indoor gatherings particularly in bars, do help stop the spread and mitigate community outbreaks. This is our country’s path forward.
The emerging data also continue to confirm the disproportionate impact of the disease on different communities, based on age, ethnicity, and race.
The Coronavirus Task Force, of which I am a member, continues to carefully analyze and monitor the prevalence of the virus throughout the U.S., using the best available science to track, predict and mitigate the curve of the outbreak. We are closely watching the entire country and working to determine the reason behind any new outbreaks or the spread of the disease.
At the FDA, our work goes beyond analyzing the numbers. Our responsibilities involve a range of efforts relating to the diagnosis, response, and treatment of COVID-19 and supporting solutions to bring an end to this crisis.
This includes facilitating the development of tests, both diagnostic and serologic, supporting the advance of treatments and vaccines for the disease, and working to ensure that health care workers and others have the personal protective equipment and other necessary medical products needed to combat it.
Since day one of this emergency, our focus in addressing these challenges has been to meet the need for speed.
To facilitate the development of new treatments and effective tests, and to make sure we have adequate supplies of essential medical equipment such as ventilators, we’ve redoubled our efforts to employ regulatory flexibility and streamlined processes where needed and appropriate, without compromising science.
The goal has been to use every available tool in our arsenal to move new treatments to patients as quickly as possible while helping ensure safety and efficacy.
We’re moving equally fast in our efforts to help support the development of COVID-19 vaccines.
As this audience is well aware, preventive vaccines for infectious disease are foundational to modern public health.
The FDA is committed to ensuring that potential vaccines for COVID-19 are safe and effective.
In June, the agency issued a guidance outlining key recommendations for vaccine development.
In particular, the agency emphasized the importance of recruiting diverse populations, especially those patients who have been disproportionately affected by the pandemic.
The FDA also recommended in the guidance that sponsors use an endpoint estimate of at least 50%, which could have an important impact on individual and public health, while vaccines with lower efficacy might not.
Several COVID-19 vaccine candidates have recently initiated large-scale clinical trials. While I cannot predict when the results from these studies will be ready, I can promise that when the data are available, the FDA will review them using its established, rigorous, and deliberative scientific review process.
We all understand that only by engaging in an open review process and relying on good science and sound data can the public have confidence in the integrity of our decisions.
One important tool we have used during public health emergencies to support the scientific investigation, is to employ our authority for Emergency Use Authorization (EUA).
An EUA allows the use of unapproved medical products or unapproved uses of approved medical products to diagnose, treat, or prevent serious or life-threatening diseases or conditions when certain criteria are met, including that there are no adequate, approved, and available alternatives.
These EUA decisions have been an important part of FDA’s efforts to shape an effective and timely response.
Though EUA decisions are based on emerging scientific evidence, we are continually evaluating and reevaluating that evidence in order to ensure that the known and potential benefits of products outweigh the known and potential risks.
Since the earliest days of the pandemic, we’ve issued EUAs for tests, ventilators, and drug treatments. The FDA has granted more than 190 EUAs for COVID-19 tests and has reviewed more than 200 clinical trials for potential therapies.
Nevertheless, we understand that the pace of FDA announcements and decisions can cause confusion for the public and providers.
For instance, some of you may be wondering whether an EUA changes the approach being used to develop drugs and vaccines. What should doctors tell their patients about what’s going on? What drugs are under development? Which are the safest or most effective?
This is a good opportunity to reiterate that although EUAs may be made on this emergency basis, they are guided by science and by continuous review of the most recent up-to-date evidence available.
Even after an EUA is issued, we regularly review that decision based on emerging information. We make any necessary changes as appropriate. This dynamic process is continually being informed by new data and evidence, and it always seeks to balance the risks with the benefits of every COVID-19 treatment.
Take testing, for example. Since day one, tests have played a key role in the ability to understand and manage this disease. Good, accurate, and reliable tests can help reveal who has the disease or, by virtue of the antibodies in someone’s system, who has been infected with the virus.
We’ve worked with hundreds of test developers, many of whom have submitted emergency use authorization requests to the FDA for tests that detect the virus or antibodies to it.
In light of the circumstances, FDA’s goal has always been to provide the necessary regulatory flexibility to support developers and to provide what patients and the public need as quickly as possible without compromising safety or scientific review.
Early on in this pandemic, the FDA posted a policy that explained that under certain circumstances, FDA did not intend to object to the use of tests that were developed and validated by laboratories prior to authorization of an EUA request. There was a national demand for such tests and we felt it was an appropriate decision to exercise regulatory flexibility concerning the use of these validated tests.
It was soon evident that some of the self-validated tests were not reliable and FDA moved quickly to update the policy in response to the available information.
Today, we have nearly 200 reliable, authorized tests. And we continue to monitor the performance of these tests and encourage the development of new and better tests that will enable us to understand this disease and help patients and the medical community address the challenges.
As we have done since the beginning of the pandemic, we will continue to balance the pressing need for access to diagnostic and antibody tests with our helping to ensure that available tests are accurate and reliable.
This same approach applies to potential treatments for COVID-19. We work closely with partners throughout the government, academia, and drug and vaccine developers to explore, expedite, and facilitate the development of products, and provide guidance and technical assistance to drug manufacturers to expedite clinical trials.
Our Coronavirus Treatment Acceleration Program, or CTAP, which we launched in March, has helped to focus the scientific and technical expertise of the agency’s staff to review potential products according to their scientific merit.
By providing enhanced regulatory support, the FDA has been able to support the initiation of more than 200 trials for COVID-19 therapies over the past few months.
This work is essential to returning us to some semblance of normalcy. After all, we need treatments and cures.
But there’s a corresponding aspect of the FDA’s work that is also essential.
This role is to support you, as physicians and medical providers to help answer your patients’ questions. Certainly, explaining the process, as complicated as it is, is an important piece of the response.
To understand this, it may be instructive to look at some actions we’ve taken with several drugs, each of which were granted an EUA, and that received significant public attention.
Back in March, the FDA granted an EUA to allow the drugs chloroquine phosphate and hydroxychloroquine sulfate to be used to treat certain hospitalized COVID-19 patients when a clinical trial was unavailable, or when participation in a clinical trial was not feasible. Early but limited research indicated that the drugs, which are approved to treat malaria and have a well-understood safety profile, might be effective in treating COVID.
After the EUA was issued, FDA continued to monitor the emerging clinical evidence on the use of these drugs in COVID-19 patients.
Based on null results from randomized controlled trials and further analysis of clinical pharmacology information, the FDA determined that chloroquine and hydroxychloroquine are unlikely to be effective in treating COVID-19 in the patient population covered by the EUA and no longer met the legal criteria for emergency use. As a result, we revoked the EUA in June.
Separately, the FDA issued an EUA for the antiviral drug remdesivir in May.
A randomized trial led by the National Institutes of Health found that remdesivir helped to reduce the length of hospitalization for COVID-19 patients. Additional trials have been completed or are planned to help us understand the appropriate role for remdesivir in this COVID crisis.
Because of the nature of the pandemic, there may be confusion or a lack of understanding about the actions we have taken on therapeutics.
We rely on you in the medical community to answer patients’ inevitable questions about treatments and vaccine development. It is our responsibility at the FDA to provide you with the information you need for your patients.
The fundamental message that we need to communicate is that the FDA’s decisions are based on science, that decisions sometimes change based on our careful review of the most recent evidence, and that we are committed to ensuring that the drugs we approve are safe and effective based on reliable data.
Physicians and other health care professionals have other important roles and responsibilities. One they share with the FDA is to help ensure that the public gets the products they are being promised and to be aware of and avoid scams being perpetrated on them.
The FDA regularly warns consumers to be cautious of websites and stores selling products with unproven claims to prevent, treat, diagnose or cure COVID-19 or unauthorized test kits. The FDA has not evaluated these fraudulent products for safety and effectiveness, and these products might actually be dangerous to patients.
To help tackle the issue of health fraud during the pandemic, the FDA launched Operation Quack Hack, which monitors online marketplaces for fraudulent products and identifies misinformation about COVID-19.
The agency has identified more than 700 fraudulent and unproven medical products related to COVID-19 and has collaborated with the Federal Trade Commission to issue warning letters to firms marketing products with misleading claims, and sent more than 150 reports to online marketplaces, and more than 250 abuse complaints to domain registrars to date.
We make most of this information available on our website and encourage doctors to become familiar with this resource and share this information with their patients.
Physicians have an important role in this area because of your ability to identify and track patients who take illegitimate or black-market drugs.
There is currently no cure for the coronavirus, and it is important for doctors to help inform patients about dangerous products and unscrupulous marketers who may be selling products with false or misleading claims.
Eight months into the pandemic, we have made important progress. Yet with cases continuing to rise, it is evident that further action is needed for our country to chart a course for recovery.
The FDA is launching the COVID-19 Pandemic Recovery and Preparedness Plan (PREPP) to help apply best practices and lessons learned from the emergency response to date. Our goal is to make needed adjustments to support the ongoing COVID-19 response, while also strengthening our resilience and improving our capacity to respond to public health emergencies in the future.
As doctors, we ensure that our treatment plans for our patients are adjusted according to the latest evidence.
I believe this same principle applies to the FDA, which as a science-based agency, is committed to continuous improvement by examining the data and modernizing our approaches when needed.
As we identify lessons and make subsequent changes, we are committed to proactively communicating any forthcoming regulatory changes to doctors and other health professionals.
Though we don’t have all the answers, we do know is that the COVID-19 virus will be with us for the foreseeable future. We are still far from understanding every aspect of this disease.
But the FDA will continue to operate with patient safety and scientific integrity as our North Star. It is this approach that continues to guide the development of new technologies and necessary regulations for safeguarding public health for the present and future.
Our goal is to provide you with the information and understanding you need to ensure that patients receive the support, attention and treatment they deserve. We look forward to working with you to achieve that goal.
- CBSE Class 10th
- CBSE Class 12th
- UP Board 10th
- UP Board 12th
- Bihar Board 10th
- Bihar Board 12th
- Top Schools in India
- Top Schools in Delhi
- Top Schools in Mumbai
- Top Schools in Chennai
- Top Schools in Hyderabad
- Top Schools in Kolkata
- Top Schools in Pune
- Top Schools in Bangalore
Products & Resources
- JEE Main Knockout April
- Free Sample Papers
- Free Ebooks
- NCERT Notes
- NCERT Syllabus
- NCERT Books
- RD Sharma Solutions
- Navodaya Vidyalaya Admission 2024-25
- NCERT Solutions
- NCERT Solutions for Class 12
- NCERT Solutions for Class 11
- NCERT solutions for Class 10
- NCERT solutions for Class 9
- NCERT solutions for Class 8
- NCERT Solutions for Class 7
- JEE Main 2024
- MHT CET 2024
- JEE Advanced 2024
- BITSAT 2024
- View All Engineering Exams
- Colleges Accepting B.Tech Applications
- Top Engineering Colleges in India
- Engineering Colleges in India
- Engineering Colleges in Tamil Nadu
- Engineering Colleges Accepting JEE Main
- Top IITs in India
- Top NITs in India
- Top IIITs in India
- JEE Main College Predictor
- JEE Main Rank Predictor
- MHT CET College Predictor
- AP EAMCET College Predictor
- GATE College Predictor
- KCET College Predictor
- JEE Advanced College Predictor
- View All College Predictors
- JEE Main Question Paper
- JEE Main Cutoff
- JEE Main Advanced Admit Card
- JEE Advanced Admit Card 2024
- Download E-Books and Sample Papers
- Compare Colleges
- B.Tech College Applications
- KCET Result
- MAH MBA CET Exam
- View All Management Exams
Colleges & Courses
- MBA College Admissions
- MBA Colleges in India
- Top IIMs Colleges in India
- Top Online MBA Colleges in India
- MBA Colleges Accepting XAT Score
- BBA Colleges in India
- XAT College Predictor 2024
- SNAP College Predictor
- NMAT College Predictor
- MAT College Predictor 2024
- CMAT College Predictor 2024
- CAT Percentile Predictor 2023
- CAT 2023 College Predictor
- CMAT 2024 Admit Card
- TS ICET 2024 Hall Ticket
- CMAT Result 2024
- MAH MBA CET Cutoff 2024
- Download Helpful Ebooks
- List of Popular Branches
- QnA - Get answers to your doubts
- IIM Fees Structure
- AIIMS Nursing
- Top Medical Colleges in India
- Top Medical Colleges in India accepting NEET Score
- Medical Colleges accepting NEET
- List of Medical Colleges in India
- List of AIIMS Colleges In India
- Medical Colleges in Maharashtra
- Medical Colleges in India Accepting NEET PG
- NEET College Predictor
- NEET PG College Predictor
- NEET MDS College Predictor
- NEET Rank Predictor
- DNB PDCET College Predictor
- NEET Admit Card 2024
- NEET PG Application Form 2024
- NEET Cut off
- NEET Online Preparation
- Download Helpful E-books
- Colleges Accepting Admissions
- Top Law Colleges in India
- Law College Accepting CLAT Score
- List of Law Colleges in India
- Top Law Colleges in Delhi
- Top NLUs Colleges in India
- Top Law Colleges in Chandigarh
- Top Law Collages in Lucknow
Predictors & E-Books
- CLAT College Predictor
- MHCET Law ( 5 Year L.L.B) College Predictor
- AILET College Predictor
- Sample Papers
- Compare Law Collages
- Careers360 Youtube Channel
- CLAT Syllabus 2025
- CLAT Previous Year Question Paper
- NID DAT Exam
- Pearl Academy Exam
Predictors & Articles
- NIFT College Predictor
- UCEED College Predictor
- NID DAT College Predictor
- NID DAT Syllabus 2025
- NID DAT 2025
- Design Colleges in India
- Top NIFT Colleges in India
- Fashion Design Colleges in India
- Top Interior Design Colleges in India
- Top Graphic Designing Colleges in India
- Fashion Design Colleges in Delhi
- Fashion Design Colleges in Mumbai
- Top Interior Design Colleges in Bangalore
- NIFT Result 2024
- NIFT Fees Structure
- NIFT Syllabus 2025
- Free Design E-books
- List of Branches
- Careers360 Youtube channel
- IPU CET BJMC
- JMI Mass Communication Entrance Exam
- IIMC Entrance Exam
- Media & Journalism colleges in Delhi
- Media & Journalism colleges in Bangalore
- Media & Journalism colleges in Mumbai
- List of Media & Journalism Colleges in India
- CA Intermediate
- CA Foundation
- CS Executive
- CS Professional
- Difference between CA and CS
- Difference between CA and CMA
- CA Full form
- CMA Full form
- CS Full form
- CA Salary In India
Top Courses & Careers
- Bachelor of Commerce (B.Com)
- Master of Commerce (M.Com)
- Company Secretary
- Cost Accountant
- Charted Accountant
- Credit Manager
- Financial Advisor
- Top Commerce Colleges in India
- Top Government Commerce Colleges in India
- Top Private Commerce Colleges in India
- Top M.Com Colleges in Mumbai
- Top B.Com Colleges in India
- IT Colleges in Tamil Nadu
- IT Colleges in Uttar Pradesh
- MCA Colleges in India
- BCA Colleges in India
Quick Links
- Information Technology Courses
- Programming Courses
- Web Development Courses
- Data Analytics Courses
- Big Data Analytics Courses
- RUHS Pharmacy Admission Test
- Top Pharmacy Colleges in India
- Pharmacy Colleges in Pune
- Pharmacy Colleges in Mumbai
- Colleges Accepting GPAT Score
- Pharmacy Colleges in Lucknow
- List of Pharmacy Colleges in Nagpur
- GPAT Result
- GPAT 2024 Admit Card
- GPAT Question Papers
- NCHMCT JEE 2024
- Mah BHMCT CET
- Top Hotel Management Colleges in Delhi
- Top Hotel Management Colleges in Hyderabad
- Top Hotel Management Colleges in Mumbai
- Top Hotel Management Colleges in Tamil Nadu
- Top Hotel Management Colleges in Maharashtra
- B.Sc Hotel Management
- Hotel Management
- Diploma in Hotel Management and Catering Technology
Diploma Colleges
- Top Diploma Colleges in Maharashtra
- UPSC IAS 2024
- SSC CGL 2024
- IBPS RRB 2024
- Previous Year Sample Papers
- Free Competition E-books
- Sarkari Result
- QnA- Get your doubts answered
- UPSC Previous Year Sample Papers
- CTET Previous Year Sample Papers
- SBI Clerk Previous Year Sample Papers
- NDA Previous Year Sample Papers
Upcoming Events
- NDA Application Form 2024
- UPSC IAS Application Form 2024
- CDS Application Form 2024
- CTET Admit card 2024
- HP TET Result 2023
- SSC GD Constable Admit Card 2024
- UPTET Notification 2024
- SBI Clerk Result 2024
Other Exams
- SSC CHSL 2024
- UP PCS 2024
- UGC NET 2024
- RRB NTPC 2024
- IBPS PO 2024
- IBPS Clerk 2024
- IBPS SO 2024
- Top University in USA
- Top University in Canada
- Top University in Ireland
- Top Universities in UK
- Top Universities in Australia
- Best MBA Colleges in Abroad
- Business Management Studies Colleges
Top Countries
- Study in USA
- Study in UK
- Study in Canada
- Study in Australia
- Study in Ireland
- Study in Germany
- Study in China
- Study in Europe
Student Visas
- Student Visa Canada
- Student Visa UK
- Student Visa USA
- Student Visa Australia
- Student Visa Germany
- Student Visa New Zealand
- Student Visa Ireland
- CUET PG 2024
- IGNOU B.Ed Admission 2024
- DU Admission 2024
- UP B.Ed JEE 2024
- LPU NEST 2024
- IIT JAM 2024
- IGNOU Online Admission 2024
- Universities in India
- Top Universities in India 2024
- Top Colleges in India
- Top Universities in Uttar Pradesh 2024
- Top Universities in Bihar
- Top Universities in Madhya Pradesh 2024
- Top Universities in Tamil Nadu 2024
- Central Universities in India
- CUET Exam City Intimation Slip 2024
- IGNOU Date Sheet
- CUET Mock Test 2024
- CUET Admit card 2024
- CUET PG Syllabus 2024
- CUET Participating Universities 2024
- CUET Previous Year Question Paper
- CUET Syllabus 2024 for Science Students
- E-Books and Sample Papers
- CUET Exam Pattern 2024
- CUET Exam Date 2024
- CUET Cut Off 2024
- CUET Exam Analysis 2024
- IGNOU Exam Form 2024
- CUET 2024 Exam Live
- CUET Answer Key 2024
Engineering Preparation
- Knockout JEE Main 2024
- Test Series JEE Main 2024
- JEE Main 2024 Rank Booster
Medical Preparation
- Knockout NEET 2024
- Test Series NEET 2024
- Rank Booster NEET 2024
Online Courses
- JEE Main One Month Course
- NEET One Month Course
- IBSAT Free Mock Tests
- IIT JEE Foundation Course
- Knockout BITSAT 2024
- Career Guidance Tool
Top Streams
- IT & Software Certification Courses
- Engineering and Architecture Certification Courses
- Programming And Development Certification Courses
- Business and Management Certification Courses
- Marketing Certification Courses
- Health and Fitness Certification Courses
- Design Certification Courses
Specializations
- Digital Marketing Certification Courses
- Cyber Security Certification Courses
- Artificial Intelligence Certification Courses
- Business Analytics Certification Courses
- Data Science Certification Courses
- Cloud Computing Certification Courses
- Machine Learning Certification Courses
- View All Certification Courses
- UG Degree Courses
- PG Degree Courses
- Short Term Courses
- Free Courses
- Online Degrees and Diplomas
- Compare Courses
Top Providers
- Coursera Courses
- Udemy Courses
- Edx Courses
- Swayam Courses
- upGrad Courses
- Simplilearn Courses
- Great Learning Courses
2 Minute Speech on Covid-19 (CoronaVirus) for Students
The year, 2019, saw the discovery of a previously unknown coronavirus illness, Covid-19 . The Coronavirus has affected the way we go about our everyday lives. This pandemic has devastated millions of people, either unwell or passed away due to the sickness. The most common symptoms of this viral illness include a high temperature, a cough, bone pain, and difficulties with the respiratory system. In addition to these symptoms, patients infected with the coronavirus may also feel weariness, a sore throat, muscular discomfort, and a loss of taste or smell.

10 Lines Speech on Covid-19 for Students
The Coronavirus is a member of a family of viruses that may infect their hosts exceptionally quickly.
Humans created the Coronavirus in the city of Wuhan in China, where it first appeared.
The first confirmed case of the Coronavirus was found in India in January in the year 2020.
Protecting ourselves against the coronavirus is essential by covering our mouths and noses when we cough or sneeze to prevent the infection from spreading.
We must constantly wash our hands with antibacterial soap and face masks to protect ourselves.
To ensure our safety, the government has ordered the whole nation's closure to halt the virus's spread.
The Coronavirus forced all our classes to be taken online, as schools and institutions were shut down.
Due to the coronavirus, everyone was instructed to stay indoors throughout the lockdown.
During this period, I spent a lot of time playing games with family members.
Even though the cases of COVID-19 are a lot less now, we should still take precautions.
Short 2-Minute Speech on Covid 19 for Students
The coronavirus, also known as Covid - 19 , causes a severe illness. Those who are exposed to it become sick in their lungs. A brand-new virus is having a devastating effect throughout the globe. It's being passed from person to person via social interaction.
The first instance of Covid - 19 was discovered in December 2019 in Wuhan, China . The World Health Organization proclaimed the covid - 19 pandemic in March 2020. It has now reached every country in the globe. Droplets produced by an infected person's cough or sneeze might infect those nearby.
The severity of Covid-19 symptoms varies widely. Symptoms aren't always present. The typical symptoms are high temperatures, a dry cough, and difficulty breathing. Covid - 19 individuals also exhibit other symptoms such as weakness, a sore throat, muscular soreness, and a diminished sense of smell and taste.
Vaccination has been produced by many countries but the effectiveness of them is different for every individual. The only treatment then is to avoid contracting in the first place. We can accomplish that by following these protocols—
Put on a mask to hide your face. Use soap and hand sanitiser often to keep germs at bay.
Keep a distance of 5 to 6 feet at all times.
Never put your fingers in your mouth or nose.
Long 2-Minute Speech on Covid 19 for Students
As students, it's important for us to understand the gravity of the situation regarding the Covid-19 pandemic and the impact it has on our communities and the world at large. In this speech, I will discuss the real-world examples of the effects of the pandemic and its impact on various aspects of our lives.
Impact on Economy | The Covid-19 pandemic has had a significant impact on the global economy. We have seen how businesses have been forced to close their doors, leading to widespread job loss and economic hardship. Many individuals and families have been struggling to make ends meet, and this has led to a rise in poverty and inequality.
Impact on Healthcare Systems | The pandemic has also put a strain on healthcare systems around the world. Hospitals have been overwhelmed with patients, and healthcare workers have been stretched to their limits. This has highlighted the importance of investing in healthcare systems and ensuring that they are prepared for future crises.
Impact on Education | The pandemic has also affected the education system, with schools and universities being closed around the world. This has led to a shift towards online learning and the use of technology to continue education remotely. However, it has also highlighted the digital divide, with many students from low-income backgrounds facing difficulties in accessing online learning.
Impact on Mental Health | The pandemic has not only affected our physical health but also our mental health. We have seen how the isolation and uncertainty caused by the pandemic have led to an increase in stress, anxiety, and depression. It's important that we take care of our mental health and support each other during this difficult time.
Real-life Story of a Student
John is a high school student who was determined to succeed despite the struggles brought on by the Covid-19 pandemic.
John's school closed down in the early days of the pandemic, and he quickly found himself struggling to adjust to online learning. Without the structure and support of in-person classes, John found it difficult to stay focused and motivated. He also faced challenges at home, as his parents were both essential workers and were often not available to help him with his schoolwork.
Despite these struggles, John refused to let the pandemic defeat him. He made a schedule for himself, to stay on top of his assignments and set goals for himself. He also reached out to his teachers for additional support, and they were more than happy to help.
John also found ways to stay connected with his classmates and friends, even though they were physically apart. They formed a study group and would meet regularly over Zoom to discuss their assignments and provide each other with support.
Thanks to his hard work and determination, John was able to maintain good grades and even improved in some subjects. He graduated high school on time, and was even accepted into his first-choice college.
John's story is a testament to the resilience and determination of students everywhere. Despite the challenges brought on by the pandemic, he was able to succeed and achieve his goals. He shows us that with hard work, determination, and support, we can overcome even the toughest of obstacles.
Applications for Admissions are open.
Aakash iACST Scholarship Test 2024
Get up to 90% scholarship on NEET, JEE & Foundation courses
ALLEN Digital Scholarship Admission Test (ADSAT)
Register FREE for ALLEN Digital Scholarship Admission Test (ADSAT)

JEE Main Important Physics formulas
As per latest 2024 syllabus. Physics formulas, equations, & laws of class 11 & 12th chapters
PW JEE Coaching
Enrol in PW Vidyapeeth center for JEE coaching
PW NEET Coaching
Enrol in PW Vidyapeeth center for NEET coaching

JEE Main Important Chemistry formulas
As per latest 2024 syllabus. Chemistry formulas, equations, & laws of class 11 & 12th chapters
Download Careers360 App's
Regular exam updates, QnA, Predictors, College Applications & E-books now on your Mobile
Certifications
We Appeared in
ORIGINAL RESEARCH article
Awareness and preparedness of covid-19 outbreak among healthcare workers and other residents of south-west saudi arabia: a cross-sectional survey.

- 1 Department of Clinical Pharmacy, Pharmacy Practice Research Unit (PPRU), College of Pharmacy, Jazan University, Jazan, Saudi Arabia
- 2 Department of Pharmacology, College of Pharmacy, Jazan University, Jazan, Saudi Arabia
- 3 Department of Pharmaceutical Chemistry, College of Pharmacy, Jazan University, Jazan, Saudi Arabia
Background: Coronavirus disease-2019 (COVID-19) was declared a “pandemic” by the World Health Organization (WHO) in early March 2020. Globally, extraordinary measures are being adopted to combat the formidable spread of the ongoing outbreak. Under such conditions, people's adherence to preventive measures is greatly affected by their awareness of the disease.
Aim: This study was aimed to assess the level of awareness and preparedness to fight against COVID-19 among the healthcare workers (HCWs) and other residents of the South-West Saudi Arabia.
Methods: A community-based, cross-sectional survey was conducted using a self-developed structured questionnaire that was randomly distributed online among HCWs and other residents (age ≥ 12 years) of South-West Saudi Arabia for feedback. The collected data were analyzed using Stata 15 statistical software.
Results: Among 1,000 participants, 36.7% were HCWs, 53.9% were female, and 44.1% were aged ≥ 30 years. Majority of respondents showed awareness of COVID-19 (98.7%) as a deadly, contagious, and life-threatening disease (99.6%) that is transmitted through human-to-human contact (97.7%). They were familiar with the associated symptoms and common causes of COVID-19. Health organizations were chosen as the most reliable source of information by majority of the participants (89.6%). Hand hygiene (92.7%) and social distancing (92.3%) were the most common preventive measures taken by respondents that were followed by avoiding traveling (86.9%) to an infected area or country and wearing face masks (86.5%). Significant proportions of HCWs ( P < 0.05) and more educated participants ( P < 0.05) showed considerable knowledge of the disease, and all respondents displayed good preparedness for the prevention and control of COVID-19. Age, gender, and area were non-significant predictors of COVID-19 awareness.
Conclusion: As the global threat of COVID-19 continues to emerge, it is critical to improve the awareness and preparedness of the targeted community members, especially the less educated ones. Educational interventions are urgently needed to reach the targeted residents beyond borders and further measures are warranted. The outcome of this study highlighted a growing need for the adoption of innovative local strategies to improve awareness in general population related to COVID-19 and its preventative practices in order to meet its elimination goals.
Introduction
An ongoing outbreak of infection by Severe Acute Respiratory Syndrome-Coronavirus-2 (SARS-CoV-2), termed as COVID-19, aroused the attention of the entire world. The first infected case of coronavirus was reported on December 31, 2019, in Wuhan, China; within few weeks, infections spread across China and to other countries around the world ( 1 ). On January 30, 2020, the World Health Organization (WHO) declared the novel coronavirus outbreak a public health emergency of international concern, which was the 6th declaration of its kind in WHO history ( 2 , 3 ). Surprisingly, during the first week of March 2020, devastating numbers of new cases were reported globally, and the WHO declared the COVID-19 outbreak a “pandemic” on March 11 ( 4 , 5 ). The outbreak has now spread to more than 200 countries, areas, or territories beyond China ( 6 ). SARS-CoV-2 is a novel strain of the coronavirus family that has not been previously identified in humans ( 7 ). The disease spreads through person-to-person contact, and the posed potential public health threat is very high. Estimates indicated that COVID-19 could cost the world more than $10 trillion, although considerable uncertainty exists concerning the reach of the virus and the efficacy of the policy response ( 8 ).
The scientists still have limited information about COVID-19, and as a result, the complete clinical picture of COVID-19 is not fully understood yet. Based on currently available information, COVID-19 is a highly contagious disease and its primary clinical symptoms include fever, dry cough, difficulty in breathing, fatigue, myalgia and dyspnea ( 9 – 11 ). This coronavirus spreads primarily through respiratory droplets of >5–10 μm in diameter, discharge from the mouth or nose, when an infected person coughs or sneezes ( 12 , 13 ). Reported illnesses range from very mild (including asymptomatic) to severe including illness resulting to death. However, the information so far suggested the symptoms as mild in almost 80% of the patients with lower death rates. People with co-morbidities, including diabetes and hypertension, who are treated with the drugs such as thiazolidinediones, angiotensin-converting enzyme (ACE) inhibitors, and angiotensin-II receptor blockers (ARBs) have an increased expression of angiotensin-converting enzyme-2 (ACE-2). Since, SARS-CoV-2 binds to their target cells through ACE-2, it was suggested that patients with cardiac disease, hypertension, and diabetes are at the higher risk of developing severe to fatal COVID-19 ( 14 , 15 ). Moreover, elderly people (≥65 years), those and people with chronic lung disease or moderate to severe asthma, who are immunocompromised (due to cancer treatment, bone marrow or organ transplant, AIDS, and prolonged use of corticosteroids or other medications), and those people with severe obesity and chronic liver or kidney disease are at higher risk of developing the COVID-19 severe illness ( 16 – 18 ).
Although, no specific vaccine or treatment is approved for COVID-19, yet several treatment regimens prescribed under different conditions are reported to control the severity and mortality rates up to some extent with few adverse effects, though further evidence is needed ( 19 ). Recently, results of ongoing trials aiming at drug repurposing for the disease have been reported, and several drugs have shown encouraging activity as far as reducing the viral load or the duration of therapy is concerned. Remdesivir is one such antiviral drug, and it has reduced the duration of therapy to 11 days in comparison to 15 days in the case of patients receiving standard care only. Therefore, the USFDA has granted the emergency use authorization (EUA) to Remdesivir for the treatment of suspected or confirmed COVID-19 cases ( 20 , 21 ); however, further investigations are required to collect the sufficient data ( 22 ). Favipiravir (Avigan) is another drug that has exhibited promising activity in significantly reducing the viral load in comparison to standard care in several trials ( 23 ). Apart from antiviral drugs, convalescent plasma for COVID-19 (as passive antibody therapy) has also been tested, proving to be of possible benefit in severely ill COVID-19 patients. However, it requires more clinical trials to be established for the optimal conditions of COVID-19 and as antibody therapy in this disease ( 24 – 26 ). Mono, and Sarilumab which are immunosuppressants and are humanized antibodies against the interleukin-6 receptor, were also tested on severely ill patients of COVID-19. They effectively improved the clinical symptoms and suppressed the worsening of acute COVID-19 patients and reduced the mortality rate ( 27 , 28 ). Very recently, a corticosteroid, Dexamethasone, has been reported to be a life-saving drug that reduced the incidences of deaths by one-third among patients critically ill with COVID-19 ( 29 ) requiring oxygen support.
So far, more than 9 million confirmed cases of COVID- 19 infections have been identified globally with more than 0.46 million confirmed deaths (as on June 21, 2020). Saudi Arabia has also been seriously affected by the COVID-19 pandemic and reported its first confirmed case on March 3, 2020. The numbers are continuously increasing and reached 157,612 on June 21, 2020, with 1,267 confirmed deaths all over the kingdom ( 30 , 31 ) having reproduction number from 2.87 to 4.9 ( 32 ). Before the emergence of COVID-19, Middle East Respiratory Syndrome-coronavirus (MERS-CoV) was the major concern in 2012 ( 33 ), though it was successfully controlled in Saudi Arabia. In response to the growing public health threat posed by COVID-19, the Saudi government adopted some unprecedented measures related to awareness and prevention in order to control COVID-19 transmission in the country. These measures included the closure of schools, universities, public transportation, and all public places as well as the isolation and care for infected and suspected cases ( 34 ). On March 9, 2020, government authorities announced the lockdown of the whole country and released advice for Saudi nationals and residents present inside or outside of country to stay at home and maintain social distancing. Moreover, the Saudi government decided to suspend congregational prayers across all mosques in the kingdom, including the two holy mosques in Makkah and Madinah ( 35 ).
The fight against COVID-19 continues globally, and to guarantee success, people's adherence to preventive measures is essential. It is mostly affected by their awareness and preparedness toward COVID-19. Knowledge and attitudes toward infectious diseases are often associated with the level of panic among the population, which could further complicate the measures taken to prevent the spread of the disease. As “natural hazards are inevitable; the disaster is not,” ( 36 ) to facilitate the management of the COVID-19 outbreak in Saudi Arabia, there is an urgent need to understand the public's awareness and preparedness for COVID-19 during this challenging time. The present study assessed the awareness and preparedness toward COVID-19 among South Western Saudi residents during the early rapid rise of the COVID-19 outbreak. It included HCWs (doctors, nurses, and community pharmacists) and other members of the community, including the employed, unemployed, as well as students.
Subjects and Methods
Setting and population.
A cross-sectional survey was conducted between March 18 and March 25—the week immediately after the announcement of lockdown in Saudi Arabia. For this study, two highly populated regions (Jazan and Aseer) of South-West Saudi Arabia and adjacent rural villages were selected. All Saudi citizens and residents, males and females of age 12 years or more (including HCWs and other community peoples), who were willing to participate in the study irrespective of COVID-19 infection status were included in the study. People who did not meet the above inclusion criteria were not eligible and were thus excluded from the study.
Sample Size
The required sample size for this study was calculated using a Denial equation ( 37 ) where the significance level (alpha) was set to 0.05 and power (1-β) was set to 0.80. It resulted in a required final sample size of 384 individuals. Therefore, to minimize the errors, the sample size taken for this study was 1,000.
Outcome Measures
The present study examined the level of awareness and preparedness toward prevention of COVID-19 using area, gender, age, education level, and occupation as explanatory variables among the residents (HCWs and other community peoples) of South-West Saudi Arabia.
Since this is a novel coronavirus with no such study having been conducted before, a standardized (structured, pre-coded, and validated) questionnaire was developed for this study by our co-authors, and it is based on frequently asked questions (FAQ) found on Centers for Disease Control (CDC) and WHO official websites ( 38 , 39 ). The questions were multiple choice and sought to gain insight into the respondent's awareness and preparedness toward COVID-19. A pilot survey of 10 individuals was undertaken first to ensure that the questions elicited appropriate response and there were no problems with the entry of answers into the database. Since, it was not feasible to conduct a community-based national sampling survey during this critical period; we decided to collect the data online through a Google survey. The self-reported questionnaire is divided into three sections. The first part is designed to obtain background information, including demographic characteristics (nationality, age, gender, level of educational, and occupation). The second part of the survey consists of questions that address awareness concerning COVID-19 (reliable source of information, symptoms, mode of transmission, incubation period, complications, high-risk population, treatment, and preventive measures). The third part of the survey consists of questions that address the preparedness to fight against COVID-19. The questionnaire is designed in English, being subsequently translated into Arabic for the convenience and ease of understanding of the participants, and it was pre-tested to ensure that it maintained its original meaning.
Data Collection and Analysis
Data were collected using a random sampling method and analyzed using the statistical software Stata 15. For categorical variables, data were presented as frequencies and percentages. A chi-squared (χ 2 ) test was used to examine the association between each item in awareness and explanatory variable in the bivariate analysis. Multivariable logistic regression was computed using each item in awareness and preparedness as an outcome separately to examine the relationships in the adjusted analysis. Differences were considered to be statistically significant at P ≤ 0.05.
Ethical Approval
The study protocol and procedures of informed consent were granted ethical approval by the “Institutional Research Review and Ethics Committee (IRREC), College of Pharmacy, Jazan University” before the formal survey was conducted. Since this study was conducted during the lockdown period, a Google survey was prepared with an online informed consent form on the first page. Participants are informed about the contents of the questionnaire, and they have to answer a yes/no question to confirm their willingness to participate voluntarily. In case of minors (participants below 16 years of age), they are asked to show the form to their parents/guardians before selecting their answer. The patients/participants or their legal guardians have to provide their written informed consent to participate in this study. After an affirmative response of the question, the participant is directed to complete the self-report questionnaire. All responses are anonymous.
Demographic Characteristics
Respondents' demographic descriptions are summarized in Table 1 . A total of 1,000 participants completed the survey questionnaire, the split being 46.1% male and 53.9% female. The majority of participants are from Jazan region (74.8%) compared to 25.2% from Aseer province. More than half (55.9%) of the participants are of <30 years of age, and 44.1% are aged ≥ 30 years. Around 79.5% respondents are university graduates holding a bachelor's degree or higher, whereas 20.5% of participants possess educational qualifications of secondary school or lower (non-graduates). HCWs make up 36.7% of participants, and 63.3% of participants are classified as other.

Table 1 . Socio-demographic characteristics of participants.
Knowledge of COVID-19 Disease and Personal Protection Measures
Table 2 displays respondents' knowledge about COVID-19, reliable sources of information, modes of transmission, symptoms of infection and complications, its perceived threat, and high-risk population. Respondents were allowed to choose more than one option from the choices given according to their understanding and conscience. The results indicated that majority of respondents had heard of and were aware of COVID-19 disease. Most of the participants (97.7%) correctly identified human-to-human transmission (contaminated person with virus) as the primary mode of transmission. Furthermore, fever, cough, and difficulty in breathing were stated as the most common COVID-19 symptoms by 89.8, 83.9, and 90.9% of respondents, respectively. The frequently reported complications of COVID-19 were pneumonia (79.4%), kidney failure (22.8%), and death (54.9%) by the respondents.

Table 2 . Awareness about COVID-19, its symptoms, transmission, and complications.
Participants' knowledge of personal protection against COVID-19 is summarized in Table 3 . The majority of respondents (76.4%) believe that there is no treatment available for COVID-19 to date, 47.1% report supportive care, and 45.8% state personal safety as the only treatment option. The most common personal protection practices adopted by participants are washing hands (92.7%), social distancing (92.3%), using a face mask (86.5%), and avoiding travel to infected areas or countries (86.9%). However, importantly, 63.8% participants believe in avoiding raw and under-cooked animal products, 16.2% choose to avoid purchasing products made in China, and 1.7% have knowledge of proper prevention methods. Approximately, half of the respondents (42.4%) report that they seek more information on COVID-19.

Table 3 . Awareness about personal protection and preparedness against COVID-19.
Preparedness to Fight Against COVID-19
Results of participants' preparedness against COVID-19 are summarized in Table 3 . Over one-third of participants are well-prepared and adopt various methods for the current situation. The majority of participants stat that they avoid crowded places, mass gatherings, or traveling to suspected areas (95.1%), and 82.7% wear face masks when going outside and have increased the use of hand sanitizers and home cleaning materials. Many of them (76.8%) now spend 20 seconds washing their hands using soap multiple times a day. However, it could be assumed from the survey that a considerable percentage of the participants do not find the protective measures necessary, visit crowded places, and do not wear face masks when leaving home.
On the other hand, HCWs also reported their preparedness on different areas to fight against COVID-19 ( Figure 1 ). All 367 (100%) HCWs who participated in this study say that they checked adequate supplies of goggles, masks, and gowns on hand for emergencies, 99.7% say they prepared links or are in contact with External Resource Centers for COVID-19 such as the CDC or WHO, 98% evaluated the patient care equipment, including portable ventilators (preparation and patient handling checklists), and 83.4% checked and prepared alternative suppliers list of certain personal protective equipment etc. Surprisingly, 18.3% of the respondents are unaware of any preparation, and 4.5% do not find it necessary.

Figure 1 . HCWs preparedness to fight against COVID 19. P1, Check adequate supplies of goggles, masks, and gowns on hand for emergencies. P2, Links to or contact External Resource Centers for COVID-19 (Coronavirus) (CDC, WHO etc.). P3, Check patient care equipment, including portable ventilators. P4, Recommendations for infection control to help biomedical and clinical engineers. P5, Check alternative suppliers of certain personal protective equipment. P6, Prepared the list to supply chain professionals. P7, Do not need any preparation. P8, I don't know.
Bivariate Analysis
The comparison between educational groups and occupational groups (HCWs vs. other residents) demonstrated significant differences in the level of knowledge and preventive measures for COVID-19 disease ( Tables 4 , 5 ). The survey shows educated participants (bachelors or more) and HCWs were more aware about COVID-19 symptoms ( P ≤ 0.001), incubation period ( P ≤ 0.001), complications ( P ≤ 0.001), high-risk populations ( P ≤ 0.01), and available treatment ( P ≤ 0.05) compared to less-educated (≤high school) ones and other residents (non HCWs). Jazan area participants heard about ( P ≤ 0.002), and showed more awareness regarding COVID-19 symptoms (fever: P ≤ 0.001), and available treatment (supportive care: P ≤ 0.001) as compared to the Aseer region. There were no significant differences found in knowledge level between gender (male vs. female) and age groups.

Table 4 . Awareness of COVID-19 stratified by occupation groups among the study participants ( n = 1,000).

Table 5 . Awareness of COVID-19 stratified by educational groups among the study participants ( n = 1,000).
Significant differences were observed in awareness about protective measures between educational groups and occupational groups ( Tables 4 , 5 ). The survey shows that the educated participants (Bachelors or more) and HCWs consider the use of face masks, frequent washing of hands, social distancing, and avoid traveling to an infected area or country as preventive measures, more so than their counter group ( P < 0.05). However, gender, age, and area comparisons on these measures were non-significant. Moreover, the survey exhibited no significant differences regarding preparedness to fight against COVID-19 level between areas, age, gender, and educational and occupational groups.
Multivariable Logistic Regressions
It was found that HCWs were more likely to be aware of COVID-19 symptoms (fever: OR = 2.15, P = 0.008; cough: OR = 1.66, P = 0.018 etc.), complications (pneumonia: OR = 2.37, P = 0.001; kidney failure: OR = 1.54, P = 0.013 etc.), populations at high risk, available treatment, and preventive measures compared to the other community members who were non-HCWs. On the other hand, less-educated participants (≤secondary schooling) were more likely to have knowledge about COVID-19 symptoms (fever: OR = 4.24, P = 0.014; breathing difficulty: OR = 2.94, P = 0.043 etc.), high-risk population (OR = 3.29, P = 0.001), complications, and preventive measures (social distancing: OR = 2.08, P = 0.008; avoid traveling to infected area or country: OR = 2.01, P = 0.002 etc.) compared to the higher-educated participants, as shown in Tables 6 , 7 . Tables displayed outcomes with statistically significant association only with explanatory variable. Area (Jazan vs. Aseer), gender (male vs. female), and age group (age <30 years vs. ≥30 years) were not associated significantly with COVID-19 knowledge. Surprisingly, no difference was reported for preparedness to fight against COVID-19 among participants.

Table 6 . Multivariable logistic regression on factors significantly associated with awareness toward COVID-19.

Table 7 . Multivariable logistic regression analysis on factors significantly associated with preventive measures toward COVID-19.
As the outbreak of COVID-19 is expanding exponentially, spreading beyond borders and spreading across continents, it has been classified as a “pandemic.” It created havoc and dismay among all nations. This new viral infection is successful in inducing restlessness, confusion, and fear among the people. The uniqueness of this infection is that it shows little or no symptoms in the beginning, and many do not even know they are infected. It does not induce any severe change or indication in the infected person so that he can seek medical attention at an early stage. By the time infected persons realize that they are infected, they might have spread the disease to a large number of people without their knowledge and any ulterior motives. Therefore, the first and foremost strategy to win the battle over COVID-19 shall be stopping the spread of disease effectively among the people. Hence, the main focus of this research was to assess the awareness of people, particularly among HCWs as well as other residents, about the disease, how they prepared themselves to fight against it, and whether they are participating in the eradication of the infection or not. We are aware that COVID-19 had taken the nation by surprise when they were least prepared to face the pandemic. To the best of our knowledge, this is the first study of its kind, conducted in Saudi Arabia that is assessing the awareness and preparedness toward COVID-19 among HCWs and other residents.
Our survey of HCWs and other residents of the study region was well-received. People of different educational backgrounds and employments participated in the survey. The majority of them are graduates, followed by people who had education up to high school. Similarly, among different employment backgrounds, HCWs make up more than one-third of the sample size. In the first place, HCWs and graduates should be aware of the disease profile, so that they can quickly spread the message among their family members, their neighbors, and all those who are within their contact. Analysis of the study results showed that both HCWs and the graduates possess adequate knowledge about the infection. It was a significant finding of our study that they can not only protect themselves against the disease but also help others to stay away from the infection by creating awareness for it. As the results suggested, health organizations (89.6%) and healthcare professionals (57.9%) are able to communicate effectively to the participants in convincing and making them understand the patterns and phases of the infection. This study also revealed that some people showed little trust in social media and other sources of communications such as television, newspaper, posters, etc. They were not convinced or accepting of the facts disseminated to them initially. It is probably for this reason that few people showed reluctance in following the guidelines given through these channels and kept ignoring them. This lack of acceptance might have accelerated the spread of this disease among the public.
Our study revealed that HCWs and people with a higher educational background (graduation or more) were more aware of the symptoms and the complications of COVID-19. It is spread via human-to-human transmission through droplet, feco-oral, and direct contact and has an incubation period of 2–14 days ( 13 ). The majority of the participants (97.7%) mentioned human-to-human contact as the primary cause of COVID-19 transmission. They were aware that the infection is related to the respiratory system, and there could be some difficulties in breathing with high temperatures accompanied by dry cough. Furthermore, it might lead to pneumonia, organ failure, and death. Indeed, COVID-19 induces these symptoms after the log period ( 40 ), although in some cases. Also, HCWs keenly follow the situation in the regions and the countries regarding the number of cases of infected and fresh cases reported daily. It perhaps helps them in getting prepared physically to manage the situation by acquiring the important things that are required in combating the disease, and it might also help them to get prepared mentally. They were aware of the social distancing, hand hygiene, using face masks, and avoiding traveling. These are the desired activities, which are expected to be practiced strictly in order to stop the spread of the disease ( 41 – 44 ). Our study revealed that HCWs and educated residents were following it meticulously. It was also known to them that no specific and effective treatment is available for COVID-19 to date, and whatever therapy is available at the designated centers is non-specific and treats only symptoms. They are sufficient enough to relieve the symptoms of the infection, to overcome difficulties in breathing, and to boost the immunity of the individuals. A similar level of awareness was reported in recent studies in China ( 10 ) and the UAE ( 45 ). This may be attributed to continuous practice of raising awareness about COVID-19 in communities about health issues by healthcare organizations and Saudi health extension workers, which has been effectively implemented in recent days ( 46 ).
Previously, MERS-CoV was a major global concern after it was first identified in 2012 in Saudi Arabia ( 33 ). Many awareness studies reported different levels of knowledge about MERS disease among Saudi HCWs and residents after the MERS outbreak ( 47 – 49 ). Present findings showed that the awareness regarding COVID-19 disease was higher compared to MERS. This can be ascribed to the global reach of COVID-19, as it is more serious than MERS owing to its high rate of transmission, alarming number of cases, and the continued global death count.
As far as preparedness to fight against COVID-19 is concerned, our study showed that all the participants were aware of avoiding mass gathering, avoiding traveling to suspected areas, the use of face masks and hand sanitizers, and maintaining proper food hygiene. During the lockdown period, the majority of the people who participated in our study stockpiled sufficient food items, and the frequency of going out to buy groceries and other food items can thus be avoided. According to them, a large number of people at supermarkets do not practice appropriate social distancing, and chances of contracting the infection might increase. This is genuinely desirable and precautionary in a situation like COVID-19, as coming closer to or violating social distancing is risky. Perhaps this preparedness is a reflection of steps taken by government authorities, as Saudi Arabia can control the spread of COVID-19 in South-West region. When the whole world is struggling to control COVID-19 spreading, Saudi Arabia has reported 1,155 positive cases (as of June 21, 2020) in Jazan and Aseer region (313 and 842, respectively) among 157,612 positive cases the entire country ( 50 ).
Also, our study confirmed that nearly half of the participants were ready to visit the hospital immediately if needed. The WHO recommends that identification of the infected individual is the first and essential step required in combating COVID-19. It also advises nations to allow citizens to get tested and put them in quarantine if they are infected. It is a significant step, as nearly 50% of the people are aware of the importance of testing in suspected cases but the remaining 50% of the participants are not. Doubts or fears about quarantine can make the public hide behind closed doors. This behavior of theirs could be dangerous, as it not only puts them in a difficult situation, but is risks their entire family and neighbors. Surprisingly, nearly 42.4% of the participants have asked for more information about COVID-19 so that they can take sufficient precautions and prepare themselves to avoid contracting the disease. These are the participants who had fewer opportunities to access healthcare services. They indeed need more information on COVID-19 to stay away from the deadly disease. This is the substantial finding of our study: nearly half of the participants did not have detailed information or a desire to gain more knowledge about the disease. The focus of the administrators should be on this category of people—the common man—so that they too can prepare themselves to fight the disease. Overall, the reported preparedness could be because the healthcare authorities have already initiated awareness and preparedness activities beyond their own borders. Every country around the world is being encouraged to draft a preparedness plan as per the WHO's global guidelines: “The ‘COVID-19' Strategic Preparedness and Response Plan” (SPRP). The SPRP outlines the public health measures that are needed to be taken to support countries to prepare for and respond to COVID-19 ( 51 , 52 ).
It was observed that the educational background plays a significant role in understanding the infection quickly. This survey showed that HCWs and people with higher education have a better understanding of the disease than their counterparts. Even though all the groups showed almost identical knowledge about the primary information of the disease, in some areas, such as disease complications, high-risk populations, personal protection measures, and treatment availability, a clear distinction exists. For example, only 68.78% of the less educated showed awareness of the high risk of contracting the infection of older people.
The WHO have initiated several online training sessions and materials on COVID-19 in various languages to strengthen preventive strategies, including raising awareness and training HCWs in preparedness activities ( 53 ). In several instances, misunderstandings among HCWs have delayed controlling efforts to provide necessary treatment ( 44 ), which led to the rapid spread of infection in hospitals ( 33 , 49 ) and putting patients' lives at risk. The present study also analyzed the preparedness of HCWs to fight against COVID-19 and found all participated HCWs were well prepared and ready for the current outbreak.
All participating HCWs report that they have adequate supplies of personal protective equipment's (PPEs), such as goggles, masks, and gowns, to manage emergencies, 99.72% of HCWs depend on an external resource center like CDC and WHO for the required emergency materials, and 98% HCWs say that they have already checked their hospitals equipped with patient care equipment, including portable ventilators. Surprisingly, few respondents (18.26%) say they were unaware of any preparation, and very few (4.36%) say that there is no need for any preparation. In general, our study indicated that the HCWs have well equipped themselves to fight against COVID-19. Although, hospitals and HCWs are fully geared up to face the pandemic situation, the best national option available is to spread awareness in order to stop the spread of disease. We have no other way but to educate our fellow citizens to not indulge in any activities that could lead them being a part of the problem. Instead, they should be encouraged to be the part of the solution.
The WHO has published guidance for public health and social measures at the workplace within the context of COVID-19. This included the standards for all workplaces and specific criteria for workplaces and jobs at medium risk and high risk. The guidance suggested to adapt the essential preventive measures for all workplaces, including practicing hand hygiene, respiratory hygiene, physical distancing (avoid direct physical contact by hugging, touching, or shaking hands), reducing and otherwise managing work-related travel, regular environmental cleaning and disinfection, risk communication, training and education, and management of people with COVID-19 or their contacts. In addition, specific measures for workplaces and jobs at medium risk included frequent cleaning and disinfection of objects and surfaces that are touched regularly (fomites). In such places where physical distancing of 1 meter cannot be maintained for a particular activity, all mitigating actions possible should be taken to reduce the risk of transmission between workers, clients or customers, contractors, and visitors, and these include staggered activities, minimizing face-to-face and skin-to-skin contact, ensuring workers work side-by-side or facing away from each other rather than face-to-face, and assigning staff to the same shift teams to limit social interaction. Along with that, such workplaces must be well-ventilated with a natural air of artificial ventilation without re-circulation of air for high-risk work activities and jobs. The WHO have advised that we find possibilities to suspend operations or adhere to the hygiene measures before and after contact with or suspicion of COVID-19. In such cases, workers must comply with the use of medical masks, disposable gowns, gloves, and eye protection for workers and use of protective equipment when in contact with COVID-19 patients, their respiratory secretions, body fluids, and highly contaminated waste. HCWs must be trained in infection prevention and control practices and use of PPEs to handle such situations ( 54 , 55 ).
The knowledge and awareness of the disease are important parameters for the adoption of protective measures that minimize the exposure risk of the illness. Our findings suggest that residents who are less educated and who are non-healthcare professionals possess less knowledge of COVID-19 disease and preventive measures than their counterparts. Therefore, health promotion and awareness programs are warranted to address these particular sections of the population. Thus, COVID-19 awareness programs and other educating strategies should be developed and implemented more effectively to eradicate this disease and increase the breadth of knowledge of rurally and minimally educated populations. These findings are useful for public health policymakers and health workers to recognize target populations for COVID-19 prevention and health education.
The strength of the study lies in its large sample size, recruited during a crucial period—the early stage of the COVID-19 outbreak in Saudi Arabia. Nevertheless, this was an online self-reported survey conducted during lockdown due to pandemic, and this affected our outreach to the general population. Our sample was obviously over-representative of well-educated people, including healthcare workers, and those who have access to computers and the internet. Hence it may not truly represent the entire population of the study region. Therefore, the generalization of the findings may suffer from reporting bias.
The present study sheds light on the current level of awareness regarding COVID 19, including knowledge, preventative practices, and preparedness in the South-West region of Saudi Arabia, which is still struggling to achieve its target of total COVID-19 eradication. The results of this survey indicated that the majority of respondents were aware of the knowledge, preventive measures and well prepared to fight against COVID-19. It was evident that the community's overall COVID-19 awareness and their preparedness among educated and HCWs populations were fairly satisfactory. However, there were few misconceptions regarding the mode of COVID-19 transmission among the participants, which need to be addressed. Knowledge and preparedness do translate into improved practices toward COVID-19 prevention and the same was reflected in this study. In order to achieve complete control over COVID-19, it would also be worthwhile to invest in various COVID-19 prevention efforts, including health education and innovative strategies based on local evidences to raise the community's awareness and to improve its preventative practices.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
RT and PT: conceptualization, methodology, writing of the original draft, investigation, project administration, and final editing. SSA and AA: supervision, co-project administration, data collection, feedback, and making substantive changes. AM: software, validation, and formal analysis. SA: visualization and investigation. WA and DB: data collection and calculations, writing, reviewing, editing of the manuscript, and formal analysis. FA: preparation of Google form and Arabic translation. All authors participated in the distribution of the survey.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We wish to acknowledge Deanship of Scientific Research, Jazan University, Jazan, Saudi Arabia, for their continuous support throughout the study.
1. Chinese Center for Disease Control and Prevention. Epidemic Update and Risk Assessment of 2019 Novel Coronavirus 2020 . (2020) Available online at: http://www.chinacdc.cn/yyrdgz/202001/P020200128523354919292.pdf (accessed February 19, 2020).
Google Scholar
2. World Health Organization. WHO Director-General's Opening Remarks at the Media Briefing on COVID-19 . (2020) Available online at: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020 (accessed March 16, 2020).
3. Muñana C, Hamel L, Kates J, Michaud J, Mollyann. The Public's Awareness of Concerns About Coronavirus . Global Health Policy. Henry J. Kaiser Family Foundation, KFF Health Tracking Poll (2020). Available online at: https://www.kff.org/global-health-policy/issue-brief/the-publics-awareness-of-and-concerns-about-coronavirus/ (accessed March 5, 2020)
4. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed. (2020) 91:157–60. doi: 10.23750/abm.v91i1.9397
PubMed Abstract | CrossRef Full Text | Google Scholar
5. World Health organization. Coronavirus Disease 2019 (COVID-19) Situation Report-51 . (2020) Available online at: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10 (accessed March 25, 2020)
6. World Health organization. Coronavirus Disease 2019 (COVID-19) Situation Report-47 . (2020) Available online at: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200307-sitrep-47-covid-19.pdf?sfvrsn=27c364a4_4 (accessed March 25, 2020)
7. Chief Executives Board for Coordination (CEB) Human Resources Network- Version 1,.0. Administrative Guidelines for Offices on the Novel Coronavirus (COVID-19) Outbreak. (2020) Available online at: https://hr.un.org/sites/hr.un.org/files/Administrative%20Guidelines%20-%20Novel%20Coronavirus%20Final_Version%201.0_13%20February%202020_0.pdf (accessed March 27, 2020)
8. Ahmed F, Ahmed N, Pissarides C, Stiglitz J. Why inequality could spread COVID-19. Lancet Pub Health . (2020) 5:e240. doi: 10.1016/S2468-2667(20)30085-2
9. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. (2020) 323:1061–9. doi: 10.1001/jama.2020.1585
10. Zhong BL, Luo W, Li HM, Zhang QQ, Liu XG, Li WT, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. (2020) 16:1745–52. doi: 10.7150/ijbs.45221
11. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. 2020 Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet . (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
12. Wu Hl, Huangc J, Casper JPZ, Zonglin H, Ming WK. Facemask shortage and the novel coronavirus disease (COVID-19) outbreak: reflections on public health measures. EClinicalMedicine . (2020) 21:100329. doi: 10.1101/2020.02.11.20020735
13. World Health organization. Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations: Scientific Brief . World Health Organization, Geneva (2020). Available online at: WHO/2019-nCoV/Sci_Brief/Transmission_modes/2020.2 (accessed April 4, 2020)
14. Fang L, Karakiulakis G, Roth M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med. (2020) 8:pe21. doi: 10.1016/S2213-2600(20)30116-8
15. Sawalha AH, Zhao M, Coit P, Lu Q. Epigenetic dysregulation of ACE2 and interferon-regulated genes might suggest increased COVID-19 susceptibility and severity in lupus patients. Clin Immunol . (2020) 215:108410. doi: 10.1016/j.clim.2020.108410
16. Chowell G, Mizumoto K. The COVID-19 pandemic in the USA: what might we expect? Lancet . (2020) 395:1093–4. doi: 10.1016/S0140-6736(20)30743-1
17. Centers for Disease Control and Prevention. People Who Are at Higher Risk for Severe Illness . (2020) Available online at: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-at-higher-risk.html (accessed March 29, 2020)
18. Bedford J, Enria D, Giesecke J. COVID-19: towards controlling of a pandemic. Lancet. (2020) 395:1015–8. doi: 10.1016/S0140-6736(20)30673-5
19. Taccone SF, Gorham J, Vincent JL. Hydroxychloroquine in the management of critically ill patients with COVID-19: the need for an evidence base. Lancet Respir Med . (2020) 8:539–41. doi: 10.1016/S2213-2600(20)30172-7
20. National Institute of Health. News Release: NIH Clinical Trial Shows Remdesivir Accelerates Recovery From Advanced COVID-19 . (2020) Available online at: https://www.nih.gov/news-events/news-releases/nih-clinical-trial-shows-remdesivir-accelerates-recovery-advanced-covid-19
21. USFDA Press Announcement. Coronavirus (COVID-19) Update: FDA Issues Emergency Use Authorization for Potential COVID-19 Treatment . (2020) Available online at: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-issues-emergency-use-authorization-potential-covid-19-treatment
22. Goldman JD, Lye DCB, Hui DS, Marks KM, Bruno R, Montejano R, et al. Remdesivir for 5 or 10 days in patients with Severe COVID-19. N Engl J Med . (2020). doi: 10.1056/NEJMoa2015301. [Epub ahead of print].
CrossRef Full Text | Google Scholar
23. Eric A., Coomes EA, Haghbayan H Favipiravir, an antiviral for COVID-19? J Antimicrob Chemother. (2020) 75:2013–4. doi: 10.1093/jac/dkaa171
24. Shen C, Wang Z, Zhao F, Yang Y, Li J, Yuan J, et al. Treatment of 5 critically ill patients with COVID-19 with convalescent plasma. JAMA. (2020) 323:1582–9. doi: 10.1001/jama.2020.4783
25. Zhang B, Liu S, Tan T, Huang W, Dong Y, Chen L, et al. Treatment with convalescent plasma for critically ill patients with severe acute respiratory syndrome coronavirus 2 infection. Chest . (2020) 158:e9–13. doi: 10.1016/j.chest.2020.03.039
26. Casadevall A, Pirofski LA. The convalescent sera option for containing COVID-19. J Clin Invest. (2020) 130:1545–8. doi: 10.1172/JCI138003
27. Xu X, Han M, Lia T, Sun W, Wang D, Fu B, et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc Natl Acad Sci USA. (2020) 117:10970–5. doi: 10.1073/pnas.2005615117
28. Regeneron Pharmaceuticals. News Release: Regeneron and Sanofi Provide Update on US Phase 2/3 Adaptive-Designed Trial of Kevzara® (Sarilumab) in Hospitalized COVID-19 Patients . (2020) Available online at: https://investor.regeneron.com/news-releases/news-release-details/regeneron-and-sanofi-provide-update-us-phase-23-adaptive (accessed June 21, 2020).
29. Randomised Evaluation of COVid-19 Therapy Trial. Statement From the Chief Investigators of the Randomised Evaluation of COVid-19 Therapy (RECOVERY) Trial on Dexamethasone: Low-Cost Dexamethasone Reduces Death by up to One Third in Hospitalised Patients With Severe Respiratory Complications of COVID-19 . (2020) Available online at: https://www.recoverytrial.net/news/low-cost-dexamethasone-reduces-death-by-up-to-one-third-in-hospitalised-patients-with-severe-respiratory-complications-of-covid-19 (accessed June 21, 2020)
30. World Health organization. Coronavirus Disease 2019 (COVID-19) Situation Report-43 . (2020) Available online at: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200303-sitrep-43-covid-19.pdf?sfvrsn=76e425ed_2 (accessed March 4, 2020).
31. World Health organization. Coronavirus Disease 2019 (COVID-19) Situation Report-153 . (2020) Available online at: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200621-covid-19-sitrep-153.pdf?sfvrsn=c896464d_2 (accessed June 21, 2020)
32. Alshammari FS. A mathematical model to investigate the transmission of COVID-19 in the Kingdom of Saudi Arabia. medRxiv . (2020) doi: 10.1101/2020.05.02.20088617
33. Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med . (2012) 367:1814–20. doi: 10.1056/NEJMoa1211721
34. Arab News. Saudi Arabia closes schools over coronavirus concerns . (2020, March 8) Available online at: https://arab.news/6g3ve (accessed March 8, 2020).
35. Arab News. Saudi Arabia suspends prayer in mosques, exempts holy Makkah and Madinah sites . (2020, March 18) Available online at: https://arab.news/yf4an (accessed March 18, 2020).
36. Jones L. The Big Ones: How Natural Disasters Have Shaped Humanity . New York, NY: Anchor Books Press.
37. Danial WW. Biostatics: A Foundation for Analysis in the Health Sciences . 7th ed., New York, NY: John Wiley & Sons (1999).
38. World Health organization. Coronavirus Disease 2019 (COVID-19) Situation Report−53 . (2020) Available online at: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200313-sitrep-53-covid-19.pdf?sfvrsn=adb3f72_2 (accessed March 25, 2020).
39. World Health Organization. Q & A on Coronaviruses (COVID-19) . (2020) Available online at: https://www.who.int/news-room/q-a-detail/q-a-coronaviruses (accessed March 19, 2020).
40. Vincent JL, Taccone FS. Understanding pathways to death in patients with COVID-19. Lancet Respir Med . (2020) 8:430–2. doi: 10.1016/S2213-2600(20)30165-X
41. World Health Organization. Coronavirus Disease (COVID-19) Advice for the Public . (2020) Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed April 13, 2020).
42. World Health Organization. Infection Prevention and Control During Health Care When Novel Coronavirus (nCoV) Infection Is Suspected . Available online at: https://www.who.int/publications/i/item/10665-331495 (accessed April 17, 2020).
43. World Health Organization. Advice on the Use of Masks in the Community, During Home Care and in Healthcare Settings in the Context of the Novel Coronavirus (2019-nCoV) Outbreak: Interim Guidance, 29 January 2020 . (2020) Available online at: https://apps.who.int/iris/handle/10665/330987 (accessed March 13, 2020)
44. Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19): Recommendation Regarding the use of Cloth Face Coverings, Especially in Areas of Significant Community-Based Transmission . (2020) Available online at: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/cloth-face-cover.html (accessed April 3, 2020).
45. Bhagavathula AS, Aldhaleei WA, Rahmani J, Mahabadi MA, Bandari DK. Knowledge and perceptions of COVID-19 among health care workers: Cross-sectional study. JMIR Public Health Surveill . (2020) 6:e19160. doi: 10.2196/19160
46. Saudi Center for Disease Prevention and Control. Coronavirus Disease 19 (COVID-19) Guidelines. V1.1 . (2020). Available online at: https://www.moh.gov.sa/CCC/healthp/regulations/Documents/Coronavirus%20Disease%202019%20Guidelines%20v1.1.pdf (accessed April 13, 2020).
47. Al-Alalawi M, Alsolami A, Alghanmi A, Said H, Alatawi A, Lhajooj A. The knowledge and attitude of King Abdul-Aziz University hospital out patient clinic visitors toward coronavirus. Egypt J Hosp Med. (2018) 70:723–7. doi: 10.12816/0043973
48. Althobaity HM, Alharthi RAS, Altowairqi MH, Alsufyani ZA, Aloufi NS, Altowairqi AE, et al. Knowledge and awareness of Middle East respiratory syndrome coronavirus among Saudi and Non-Saudi Arabian pilgrims. Int J Health Sci. (2017) 11:20–5.
PubMed Abstract | Google Scholar
49. Kharma MY, Alalwani MS, Amer MF, Tarakji B, Aws G. Assessment of the awareness level of dental students toward Middle East Respiratory Syndrome-coronavirus. J Int Soc Prev Community Dent. (2015) 5:163–9. doi: 10.4103/2231-0762.159951
50. COVID 19 Dashboard: Saudi Arabia . Available online at: https://covid19.moh.gov.sa/ . (accessed on June 21, 2020)
51. World Health Organization. COVID-19 Strategic Preparedness and Response Plan . (2020) Available online at: https://www.who.int/docs/default-source/coronaviruse/srp-04022020.pdf (accessed on March 26, 2020).
52. World Health Organization. 2019 Novel Coronavirus (2019-nCoV): Strategic Preparedness and Response Plan . (2020) Available online at: https://www.who.int/docs/default-source/coronaviruse/srp-04022020.pdf (accessed March 26, 2020)
53. World Health Organization. Coronavirus Disease (COVID-19) Training: Online Training . (2020) Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/training/online-training (accessed on April 12, 2020).
54. World Health Organization. Considerations for Public Health and Social Measures in the Workplace in the Context of COVID-19: Annex to Considerations in Adjusting Public Health and Social Measures in the Context of COVID-19 . 10 May, 2020. (2020) Available online at: https://www.who.int/publications/i/item/considerations-for-public-health-and-social-measures-in-the-workplace-in-the-context-of-covid-19 (accessed June 16, 2020)
55. Cirrincione L, Plescia F, Ledda C, Rapisarda V, Martorana D, Moldovan RE, et al. COVID-19 pandemic: prevention and protection measures to be adopted at the workplace. Sustainability . (2020) 12:3603. doi: 10.3390/su12093603
Keywords: COVID-19, coronavirus, outbreak, awareness, preparedness, healthcare, residents, questionnaire
Citation: Tripathi R, Alqahtani SS, Albarraq AA, Meraya AM, Tripathi P, Banji D, Alshahrani S, Ahsan W and Alnakhli FM (2020) Awareness and Preparedness of COVID-19 Outbreak Among Healthcare Workers and Other Residents of South-West Saudi Arabia: A Cross-Sectional Survey. Front. Public Health 8:482. doi: 10.3389/fpubh.2020.00482
Received: 15 May 2020; Accepted: 28 July 2020; Published: 18 August 2020.
Reviewed by:
Copyright © 2020 Tripathi, Alqahtani, Albarraq, Meraya, Tripathi, Banji, Alshahrani, Ahsan and Alnakhli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY) . The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pankaj Tripathi, pankaj10pcol@gmail.com
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Mobile Menu Overlay
The White House 1600 Pennsylvania Ave NW Washington, DC 20500
Remarks by President Biden at the Global COVID- 19 Summit
Residence Library
(Prerecorded)
THE PRESIDENT: Hello, everyone. Thank you for joining together for the second Global COVID-19 Summit. You know, and a special thank you to the leaders of Belize, Germany, Indonesia, Senegal for — for cohosting this summit with the United States. Today, we’re again uniting countries around the world with leaders from the private sector, civil society, and the philanthropic community to carry forward the vital work on fighting COVID-19 everywhere — not just at home, everywhere. You know, when we met last, in September, we were focused on critical and urgent challenges. And I’m incredibly proud of the work that have — that we’ve done together over the last several months and the commitments that we made — have made to — to vaccinate the world. You know, for our part, the United States has provided more than $19 billion to help countries fight COVID-19 all around the world. We’ve provided lifesaving medicines, oxygen, tests, equipment, supplies, and partnered with countries to improve their capacity to manufacture vaccines as well. We’ve delivered more than 500 million vaccines to 115 different countries. And we’re going to continue to work with COVAX to deliver another 500 million doses — all part of the pledge we made to donate 1 billion doses of vaccine to the most vulnerable in the world. You know, all — you know, all this is completely free. No — no strings attached.
But, you know, there’s still so much left to do. This pandemic isn’t over. Today, we mark a tragic milestone here in the United States: one million COVID deaths, one million empty chairs around the family dinner table — each irreplaceable. Irreplaceable losses, each leaving behind a family, a community forever changed because of this pandemic. My heart goes out to all of those who are struggling, asking themselves, “How do I go on without him?” “How do I go on without her?” “What will we do without them?” It’s grief shared by people across all of our nations. Around the world, many more millions have died. Millions of children have been orphaned. And with thousands still dying every day, now is the time for us to act — all of us — together. We all must do more. We must honor those we have lost by doing everything we can to prevent as many deaths as possible. Today, we’re at a new stage in fighting this pandemic, facing an evolving set of challenges. We have to double down on our efforts to get to — get shots in people’s arms, country by country, community by community; ensure we have reliable and predictable supplies of vaccines and boosters for everyone, everywhere; expand access globally to tests and treatments; and we have to prevent complacency. This summit is an opportunity to renew our efforts, to keep our foot on the gas when it comes to getting this pandemic under control and preventing future health crises. Collectively, we are making significant new commitments to help keep up the fight against COVID-19 in 2022, protect the most vulnerable populations, and prepare for the next health crisis, because there will be others. You know, and the United States is going to continue to do our part. Today I’m announcing the United States will share critical COVID-19 technologies through the World Health Organization COVID-19 Technology Access Pool. We’re making available health technologies that are owned by the United States government, including stabilized spike protein that is used in many COVID-19 vaccines. We’re standing up a new pilot program, working with the Global Fund, to expand access to rapid testing and antiviral treatments for people in harder-to-reach areas. And we’re increasing our support for a new Pandemic Preparedness and Global Health Security fund that will be established at the World Bank this summer with $450 million in seed funding. I particularly want to commend Indonesia and Italy for their leadership in helping make this fund a reality. And I’m encouraging other leaders to join me in — in upping their commitments. You know, we’re going to face, together, global health crises. This is not the last one we’ve had. It’s not a question of “if,” it’s a question of “when.” So we have to invest now. Now. We have to secure political commitments now. We have to start working to prevent the next variant and the next pandemic now. And that’s — and, you know, that’s going to require all of us — all of us to do more. I encourage every leader to ask yourself, “What more can I do? How can we work more closely together to help more people? How can we save more lives?” That’s why I continue to call on Congress here at home to take the urgent action to provide emergency COVID-19 funding that is vital to protect Americans, to make sure we’re — that we maintain our — our supplies of COVID-19 tests, treatments, and vaccines, including next-generation vaccines that are being developed. The request also includes $5 billion to keep up our global partnership in the fight against COVID-19 and sustain our efforts to get ever- — get shots in people’s arms all around the world, expand access to treatment, and save lives everywhere. We can do this. We can control COVID-19. We can start to build a better, healthier, and more secure future today if we all do our part and if we step up together. So thank you for responding to this fight. And most especially, thank you for all the doctors, nurses, and community health workers, and scientists, and aid workers, and anyone and everyone on the frontlines fighting this pandemic, saving lives every single day. We owe you. Thank you. And God bless you all. END
Stay Connected
We'll be in touch with the latest information on how President Biden and his administration are working for the American people, as well as ways you can get involved and help our country build back better.
Opt in to send and receive text messages from President Biden.
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- My Account Login
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Open access
- Published: 01 February 2022
Persuasive narrative during the COVID-19 pandemic: Norwegian Prime Minister Erna Solberg’s posts on Facebook
- Sanjana Arora ORCID: orcid.org/0000-0003-0107-7061 1 ,
- Jonas Debesay 2 &
- Hande Eslen-Ziya ORCID: orcid.org/0000-0001-7113-6771 1
Humanities and Social Sciences Communications volume 9 , Article number: 35 ( 2022 ) Cite this article
7236 Accesses
5 Citations
5 Altmetric
Metrics details
- Cultural and media studies
- Politics and international relations
This article explores the Facebook posts of Norway’s Prime Minister Erna Solberg to highlight the key features of her crisis communication during the COVID-19 pandemic. It draws on data from Solberg’s Facebook posts from February 27, 2020 to February 9, 2021 (i.e., starting from the day when the first case of COVID-19 was recorded in Norway until the time of data collection for this study). Out of her 271 posts, 157 of them were about COVID-19 and were chosen for analysis. The analyses identified five major themes: (1) Promoting responsibility and togetherness (2) Coping (3) Being in control amidst uncertainty (4) Fostering hope and (5) Relating with the followers. Drawing inspiration from Boin, Stern and Sundelius’, work on persuasive narratives, this study shows the ways that Solberg’s posts about COVID-19 exhibit all five identified frame functions. In addition, the findings add contextual nuances to the frame functions through the theme of ‘Responsibilization and togetherness’, which are reflected through references to Norwegianness and the cultural concept and practice of dugnad . This study adds to our knowledge about how persuasive narratives are incorporated into the social media communication strategies of leaders and highlights the usefulness of this framework for studying ongoing and future crises.
Similar content being viewed by others

Slovak MPs’ response to the 2022 Russian invasion of Ukraine in light of conspiracy theories and the polarization of political discourse

The gendered dimensions of the anti-mask and anti-lockdown movement on social media

Constructing collective identities and solidarity in premiers’ early speeches on COVID-19: a global perspective
Introduction.
The economic and social disruption caused by the COVID-19 pandemic is having major impacts on people’s livelihoods and their health. As of 18 April 2021, there have been 140,322,903 confirmed cases of SARS-CoV-2 infections and 3,003,794 deaths (WHO, 2021 ), making the COVID-19 pandemic an unprecedented global health crisis of the century. As countries across the world grapple with mitigating the risks associated with the pandemic, communication—an essential component of planning, response, and recovery during crisis (Houston et al., 2014 )—has been one of the integral parts of the crisis management (Reddy and Gupta, 2020 ). Crisis communication highlights legitimation strategies, but also indicates how government institutions themselves make sense of crises (Brandt and Wörlein, 2020 ). Moreover, crises such as the COVID-19 pandemic can disrupt the socio-political order of societies, leaving a cognitive void in the minds of the public that can be filled with fear and uncertainty (Boin et al., 2016 ). In Norway, COVID-19 has been called a fear-driven pandemic that is based on alarming information of long-term illness and disability that is out of politicians control (Vogt and Pahle, 2020 ). Having control over the dramaturgy of political communication is thus central to effective leadership and crisis management (Boin et al., 2016 ). Effective communication can help societies handle uncertainty and promote adherence to behaviour change while fostering hope among the citizens (Finset et al., 2020 ).
The COVID-19 pandemic continues to rapidly evolve, and social media plays a pivotal role in meeting the communication needs of the public during such crisis (Van Dijck, 2013 ). As social media use increases during crises, leaders and public officials may utilise this platform to communicate, which in return helps reduce public panic and builds trust (Kavanaugh et al., 2012 ). As a result of the cultural and symbolic value of social media in contemporary times (Jenzen et al., 2021 ), the communication of public leaders in the midst of uncertainty and fear facilitates interpersonal and group interaction. Research has shown that, when compared to the traditional media platforms, social media platforms are used by leaders and elected officials to communicate, inform, and engage with their citizens (Golbeck et al., 2010 ). They use social media to spread messages farther and faster than it would be possible with traditional media (Sutton et al., 2013 ). What leaders post on social media can give insights into their communication and leadership strategies during crises. Understanding how leaders communicate with the public during crises will not only provide us with the knowledge about their governance styles but will also guide us to their meaning-making in times of uncertainty. Based on this assumption we will be studying the Facebook posts of Norwegian Prime Minister Erna Solberg, with the aim to highlight the key features of her communication. In doing so, we will take an exploratory rather than confirmatory perspective (Boudreau et al., 2001 ).
Solberg, member of the Conservative Party and in power since 2013, was defeated by the centre-left as this paper was being revised. Solberg has had a long career in politics, becoming a deputy representative to the Bergen City Council in 1979 when she was 18 years old. She was elected to the Parliament in 1989 where she was the youngest member of her party group (Notaker and Tvedt, 2021 ). Solberg’s tough stance on issues such as immigration earned her the nickname of ‘Jern-Erna’ [Iron Erna] (Reuters, 2013 ). However, upon her appointment as Prime Minister, Solberg displayed a ‘softer side’ by caring about voters’ jobs, health, and schools (Notaker and Tvedt, 2021 ).
The first Norwegian COVID-19 patient was diagnosed on February 26, 2020. While the initial spread of infection was relatively slow, cases increased quickly by March 12 th , after winter break for schools ended and many Norwegians returned from skiing holidays in Northern Italy (Dagsavisen, 2020 ). On March 12, the Norwegian Directorate of Health (NDH) adopted comprehensive measures to prevent the spread, which included closing day care centres, schools, and educational institutions. The measures also included a ban on cultural events, closed swimming gyms and pools, a halt to all service provisions that involved being less than one meter away from another person, and prohibiting visits to recreational cabins Footnote 1 , among others. Behavioural measures such as recommendations to keep physical distance, encourage handwashing, quarantine, stay home when ill, work from home, and avoid public transportation were also included. Following the lockdown, Norway became the first European country to announce that the situation was under control due to low levels of hospitalizations and mortalities (Christensen and Lægreid, 2020 ). In Norway, as of March 22, 2021, there have been over eighty thousand confirmed cases of coronavirus infection and more than six hundred deaths due to COVID-19. Norway has had far fewer COVID-19 cases, deaths, and hospitalizations per capita than most other countries in Western Europe or the United States (Christensen and Lægreid, 2020 ). Compared to its Scandinavian neighbours Denmark and Sweden, the proportion of cases of infections and deaths have been much lower (WHO, 2021 ), despite the three countries sharing similar social welfare and healthcare systems. Recently, a report submitted by the Corona Committee in Norway also concluded that the overall handling of the crisis by the government has been good. Not only has the number of infections and deaths in Norway been much lower than most countries in Europe, but the healthcare services have also remained stable, and society has remained relatively open (Lund, 2021 ). It is probable that good governance and responsible leadership demonstrated by the Norwegian cabinet and Prime Minister Erna Solberg contributed to this success.
In Norway, there is considerably less focus on individualization of candidates in political parties as compared to for instance the US, since the electoral system in Norway is based on proportional representation (Karlsen and Enjolras, 2016 ). Despite this, with the presence of digital and social media, there has been increasing focus on the individual candidates, leading to ‘decentralising personalisation’ (Karlsen and Enjolras, 2016 ; Balmas et al., 2014 ). Given this context, Erna Solberg’s Facebook account during the COVID-19 pandemic serves as an intermediary platform between the government’s role and her own personal profile as the Prime Minister who has been handling the COVID-19 crisis. Solberg has used Facebook more actively than other outlets like Twitter and has more followers on Facebook than any other platform. The proportion of Facebook users in Norway vis-a-vis other social media platform is also the highest (for example, 84% of people use Facebook compared to 22% who use Twitter who use Twitter) (Werliin and Kokholm, 2016 ). Facebook thus serves as an important platform for public leaders in Norway during crises, and therefore, by analysing Solberg’s Facebook posts, we aim to demonstrate the key features of her communication strategy during the COVID-19 crisis.
Background on crisis and crisis communication
Crisis is defined as a rare, and significant public situation creating undesirable consequences (Coombs, 2015 ; Gruber et al., 2015 ). In most cases it is ‘an unpredictable event that threatens important expectancies of stakeholders and can seriously impact an organization’s performance and generate negative outcomes’ (Coombs, 2015 : p. 3). Crisis communication on the other hand is referred as the strategies used to lessen the uncertainties during crisis via the dissemination and exchange of information (Collins et al., 2016 ). Effective crisis communication establishes reliability and maintains public trust. It should be frequent, consistent and involve compassionate messages conveyed in an inspired and transformational communication style. It is essential that public officials and leaders when communicating crisis relevant information be efficient and informative. Past research has shown the importance of repetition of the consistent interaction to help the message reach the recipients clearly and increase compliance behaviour in cases of crisis (Stephens et al., 2013 ). Inconsistent messages on the other hand were found to cause misperception and confusion, leading to a non-compliant behaviour by the recipients. The content of the message as well as its tone is also an important indicator of whether the recipients will comply or not (Sutton et al., 2013 ). Sources of crisis communication, such as leaders and public health officials, are perceived to be reliable and trustworthy when they exhibit concern and care (Heath and O’ Hair, 2010 ). In addition, they can be more effective in building relationship with the public, if they consider the cultural factors that play a role in their communicating about risks (Aldoory, 2010 ).
Boin et al. ( 2016 ) argue that crisis communication is one of the key challenges, which leaders face during a crisis situation. During crisis communication, leaders are required to frame ‘meaning’ of the crisis in order to shape how public perceives the risks, consequences and how they respond to the measures being taken. Developing a persuasive narrative in communication is thus integral to succesful framing of the crisis and for a strategic leadership. The construction of a successful persuasive narrative requires five frame functions: namely that the narrative will offer a credible explanation of what happened, it will provide guidance, instil hope, show empathy, and suggest that leaders are in control (Boin et al., 2016 ). In doing so, leaders aid the public’s understanding of the facts associated with crisis while sumltaneously acknolwedging and appealing to collective emotions. In incorporating these frame functions, leaders are posed with various choices and decision-making such as how they choose to or not choose to dramatise the situation, the language that they use and how they appeal to the colleactive emotions and stress.
As digital media technologies became popular resources for getting and spreading information, public officials and leaders also increasingly started using them as domains during the crises. In fact, for some scholars the use of social media while enabling mutual interaction between the leaders and recipients has altered the field of crisis communication altogether. For instance, it was found that as social media enables constant and effective communication, it was used more regularly than traditional media outlets during crisis (Kim and Liu, 2012 ). Similarly, Utz et al. ( 2013 ) discussed how for effective crisis communication strategy, the use of media channels, social media—Twitter, and Facebook—versus traditional— newspapers—was more critical than the type of the crisis. Moreover, Schultz et al. ( 2011 ) concluded that when compared to traditional media networks, crisis communication received less negative response when social media was used. Hence, it is not to our surprise that public officials nowadays are turning to social media platforms for communicating with the masses during crisis. They not only use these tools to communicate about crisis but also request information from the public. This was the case during the COVID-19 pandemic crisis where social media was employed by political leaders across the globe to mediate the communication of information about the pandemic as well as for reaching out to their citizens. This paper by focusing on the Norwegian case and more specifically on the Norwegian Prime Minister’s Facebook use during the time of COVID-19 pandemic aims to explore the use of social media platforms by political leaders during crisis. Our goal is to better understand how political leaders adapt social media technologies in their communication strategies during crises.
Our data that covers Erna Solberg’s Facebook posts between February 27, 2020, and February 10, 2021 (a total of 271 posts) were extracted from Footnote 2 into an Excel sheet. A total of 114 posts were removed as they were not related to COVID-19 leaving us 157 posts for further analysis. To aid the coding process, we noted the variables presented in Table 1 . These are: date, number of interactions, number, and type of reactions (e.g., angry, sad, like, etc.), URLs of links shared, and a description of the content of the posts that was later used in the qualitative analysis. We also noted if the posts were made during any particularly critical period (e.g., before, during or after new restrictive measures were introduced). The content of the posts and the number of likes and other reactions derived from this data should be considered a ‘snapshot’ of Solberg’s posts as they appeared at the time of data collection (Brügger, 2013 ), as it is possible that some posts have been subsequently removed, or that the numbers and types of reactions to the posts have changed by the publication date
The data was analysed through thematic analysis (Braun and Clarke, 2006 ): in the first step, we read all posts and generated the first set of codes. Next, we combined all the similar codes while labelling them in clusters and organised them into analytical themes/categories (see Fig. 1 ). The authors then discussed and reviewed these analytical themes and merged them into aggregate/conceptual themes. Lastly, we reviewed the aggregate themes through the lens of the five frame functions of persuasive narrative and identified commonalities and differences. We have included some posts under each theme to illustrate our analytical process and illuminate the themes (Sandelowski, 1994 ). All posts presented here were translated from Norwegian to English by the authors.

Schematic formulation of a theme from the categories captured in posts.
Our analysis resulted in five themes: (1) Promoting responsibility and togetherness (2) Coping (3) Being in control amidst uncertainty (4) Fostering hope and (5) Relating with the followers. In reviewing our findings from the framework of Boin et al. ( 2016 ), we found that all five frame functions of persuasive narrative were embedded in Solberg’s posts and aligned with our themes. Below we discuss our themes with reference to frame functions of Boin et al. ( 2016 ) for a persuasive narrative and in doing so, add contextual nuances to each theme.
Promoting responsibility and togetherness: we are in this together
Analysis of Solberg’s posts revealed a strong message of responsibility and togetherness. In almost all shares, she not only emphasized solidarity but also called for courage and responsibility. This Facebook post, shared soon after comprehensive shut-down measures were introduced, shows how important, for Solberg, was Norwegian solidarity expressed as ‘we’ (March 12, 2020):
Dear everyone. In times of crisis, we understand how dependent we are on each other. What unites us is more important than what separates us. This is not the time for ‘I’. This is the time for ‘we’.
Lunn et al. ( 2020 ) note that citizens are isolated during government induced or self-imposed quarantines: appeals to collective action and a spirit of ‘we-are-in-it-together’ are important ways to ensure compliance with quarantine and hence curb the rate of infection. Leaders in countries such New Zealand, UK, Brazil have also been found to have used a similar narrative emphasizing patriotic duty, love of country, and coming together as one, to mobilise community action (Dada et al., 2021 ).
Her posts were also imbued with appreciation and expression of gratitude towards healthcare workers and those who follow rules. For example, after introduction of the ban to travel to cabins and after the government’s decision to extend regulations until after Easter, Solberg posted the following on April 4, 2020, receiving a high number of likes:
I feel proud when I see how we handle this together. Many thanks to everyone who follows the advice from the health authorities. Many thanks to everyone in the health service who works hard and perseveres. Many thanks to all Norwegians for the patience, love and solidarity we now show each other
The use of the word ‘I’ and how it was being used in reference to ‘feel[ing] proud’, we argue, highlights the ‘positioning of self’ by Solberg. Davies and Harré ( 1990 ) claim that development of the notion of ‘positioning’ is a contribution to the understanding of personhood, and how speakers choose to position their personal identity vis-a-vis their discontinuous personal diversity (such as being the Prime Minister, politician, Norwegian citizen, etc.). In such posts, whether intentionally or unintentionally, we also see the discursive practices through which Solberg allocates meaning to her position as a Prime Minister by emphasising that she feels proud upon seeing those who follow advice. At the same time, her emphasis on ‘we’, as in how ‘ we handle this together’, places her as a member of the Norwegian masses.
Moreover, such references to togetherness and solidarity also reflect attempts to utilise the existing nationalistic cultural repertoire of the Norwegian concept of dugnad . For example, on New Year’s Day following the Gjerdrum community disaster (a sudden and unexpected mudslide that destroyed several residential houses) and rise in the number of infections during the holiday period (2125 reported cases on December 29, 2020), Solberg posted the following post:
[…] During the year we have put behind us, Norway has lined up for the big dugnad . People have put their interests and dreams on hold to protect the elderly and the risk groups. It has saved lives. I am deeply grateful, proud and touched, for the way the Norwegian people have handled the biggest challenge for our society since World War II. We lined up for each other when it mattered most…
Dugnad in Norwegian is voluntary work that is performed as a collective effort (Moss and Sandbakken, 2021 ). Nilsen and Skarpenes ( 2020 ) discuss how the concept of dugnad is embedded in a moral repertoire of the socially responsible citizen that is indicative of a specifically Norwegian welfare mentality and conclude that dugnad is imperative for the sustainability and resilience of the Norwegian welfare model. Before the pandemic, Simon and Mobekk ( 2019 ) argued that the concept of dugnad is central to Norwegian culture, inculcating prosocial and cooperative behaviour, and thereby plays a role in Norway being one of the most egalitarian democracies and having high levels of equality and reciprocity. In the context of COVID-19, social anthropologist Thomas Hylland Eriksen ( 2020 ) pointed out that one reason for the success of the Norwegian approach was the mobilisation of broader society to fight COVID-19, driven by the notion of dugnad . Similarly, Moss and Sandbakken ( 2021 ) analysed data from press conferences and interviews with members of the public and found that many participants mentioned liking how the government talked of ‘a spirit of dugnad ’ ( dugnadsånd ), appealing to shared voluntary work rather than strict rules. The authors posit that in a pandemic it is crucial to create and use meta-narratives that are a good fit with the context in order to aid meaning-making and increase compliance. The use of dugnad as a cultural repertoire has, however, met with criticism from some scholars, who argue that ‘a word associated with solidarity, unity, and voluntary work obscures the forced nature of the measures’ (Tjora, 2020 ) and shifts the onus for finding solutions onto individual citizens or groups (Nilsen and Skarpenes, 2020 ; Hungnes, 2016 ).
Despite the criticism of imbibing such cultural repertoire, the alignment of the key values of Norwegian society with the core message of encouraging collective action is essential for a crisis narrative to be politically effective (Boin et al., 2016 ). Furthermore, the theme of ‘Promoting responsibility and togetherness’ shows the context specific nature of crisis communication narrative in the case of COVID-19 in Norway and therefore adds to the components for a persuasive narrative.
Coping: everything will be fine
Solberg’s Footnote 3 posts also carried messages that address the consequences of coping with COVID-19, namely self-isolation, and loneliness. For instance, her posts guided followers in dealing with loneliness and maintaining general physical and mental health. The Norwegian government, like that of many other countries, had introduced measures such as mandatory quarantine and social distancing rules to manage the spread of the virus. Studies have shown that home confinement during COVID-19 has negatively affected the emotional state of individuals due to depression and anxiety and has led to or increased a sedentary lifestyle (Sang et al., 2020 ). Thus, emphasis on the well-being of the population during COVID-19 is important for effective crisis management (WHO, 2020a ) because increased well-being would reinforce its coping abilities during illness and hardships. As these are not the direct effects of the COVID-19 infection, but a result of the contagion containment measures imposed on citizens by the government, we observe Solberg taking responsibility and providing solutions to help. In doing so, she appears sensitive and caring towards the public.
Christensen and Lægreid ( 2020 ) attribute the ‘high-performing’ handling of the pandemic in Norway to the initial focus on suppression, followed by a control strategy. The authors further examine the ideas that having successful communication with the public, a collaborative and pragmatic decision-making style, the country’s resourcefulness, and high trust of government all contributed to the relative success in Norway. Adopting the correct and effective strategy indeed heavily influences the outcomes of crises. However, to fill the ‘cognitive void’ that the public might be experiencing, leaders need to manage the meaning-making process and ensure legitimacy of their actions (Boin et al., 2016 ). Solberg and the other ministers played an important role in communicating with citizens and the media through daily media briefings together with the NDH (Norwegian Directorate of Health) and NIPH (Norwegian Institute of Public Health) (Christensen and Lægreid, 2020 )
Solberg emphasized the impact of loneliness, for example, during one of the first holiday periods during the pandemic when comprehensive shut-down measures were introduced, she wrote:
Many people may feel lonely during holidays such as Easter, and the corona crisis exacerbates this. Therefore, I would like to encourage everyone to call someone you know is alone at Easter. The little things can mean a lot. Happy Easter!
A study by Blix et al. ( 2021 ) on the topic of mental health in the Norwegian population during the COVID-19 pandemic found that a substantial proportion of the population experienced significant psychological distress in the early phases. More than one out of four reported ongoing psychological distress over the threshold for clinically significant symptoms. Two other categories of individuals (those recently exposed to violence and those with pre-existing mental health problems) were found to be at special risk but worrying about the consequences of the pandemic was also found to contribute negatively to mental health. In this regard, Shah et al. ( 2020 ) argued that several nations have failed to address the mental health aspect among the public, as far more effort is being focused on understanding the epidemiology, clinical features, transmission patterns, and management of COVID-19. Solberg’s open discussion about mental health during the pandemic implies a situation-specific and data-driven strategy of managing the less visible effects of the pandemic and show insight in anticipating future needs (Han et al., 2020 ).
Moreover, Solberg’s posts also subtly utilised the Norwegian concept of friluftsliv , which translates as ‘free air life,’ a philosophy of outdoor living and connection with nature (Henderson and Vikander 2007 ). Friluftsliv is associated with grand narratives of Norwegian national identity depicting outdoor adventures, foraging, and a deep connection to nature (Jørgensen-Vittersø, 2021 ). For example, with the re-opening of DNT [Den Norske Turistforening] cabins in mid-2020, Solberg in her post on June 11 emphasized the importance of being outdoors in fresh air:
We need to use our bodies and get out into the light and fresh air. It is important for both physical and mental health! I hope many have a good and active Norwegian holiday this year!
In these posts, Solberg also shared pictures of herself being outdoors. In such ways, Solberg appeared to be offering not only guidance for coping with the challenges and consequences of living during the pandemic, but also emphasizing one characteristic of the Norwegian culture, which they are proud of—spending time in nature. Be it advice to spend time in nature, or to keep social distance or self-isolation, we consider that Solberg’s approach to coping aligns with the frame function of ‘offering guidance’. During a crisis, leaders have a window of opportunity during which they can communicate a frame to not only make sense of the crisis but also to provide guidance and to portray themselves as attentive and concerned about the challenging circumstances faced by the public (Boin et al., 2016 ). By depicting herself as attuned to the emotions experienced by her followers during the pandemic and by utilising the moment to suggest ways of coping, Solberg’s communication encapsulates the frame function of offering guidance for a persuasive narrative.
Being in control amidst uncertainty
In her posts, Solberg presented a narrative of being in control amidst uncertainty, which aligns with two of the frame functions of Boin et al. ( 2016 ), namely offering a credible explanation and suggesting that leaders are in control. In times of a crisis, it is important that leaders do not downplay the gravity of the situation or claim unrealistically optimistic scenarios (Boin et al., 2016 ). We see that Solberg maintained a balance by providing a detailed explanation of her actions and the reasons behind the restrictive measures taken. At the same time, she acknowledged the uncertainty inherent in the ever-changing crisis and demonstrated her concern. According to Lunn et al. ( 2020 ), in situations characterised by uncertainty and fear, responsible leaders need to signal that they are in control of the situation, which can be demonstrated by making decisions with confidence and honesty. Moreover, it is also essential that leaders do not make promises that are impossible or unrealistic, because doing that can impede the persuasiveness of their narrative by affecting their credibility later (Boin et al., 2016 ). In Solberg’s posts, we see that she displays confidence but also the reality of uncertainty and concern, which is a sign of effective leadership and shows ‘bounded optimism’ (Brassey and Kruyt, 2020 ). The following post where she writes about her worries and concerns followed by advice is a good example of credibility and control:
I am worried. Right now, we have ongoing outbreaks in Bergen, Oslo, Trondheim and Hammerfest… We know that vigorous work is being done intensively in these municipalities with infection detection and other measures. Although Norway has relatively low infection rates, we also register here at home that the number of hospital admissions and the number of infected have increased recently. We now have the highest number of hospitalized patients with COVID-19 since May… We also see that the infection has begun to spread to older age groups. And there is a significant risk that the numbers will continue to rise as we see in Europe. That is why we have today announced new national austerity measures next week. We can still reverse the trend here at home…
A demonstration of concern from role models has been shown to have a role in persuading the public to adhere to recommendations (Simon and Mobekk, 2019 ). Tannenbaum et al. ( 2015 ) note that fear is easier to handle when it is acknowledged, which relates to the idea of ‘citizens being anxious enough to take the advice from the authorities to heart and optimistic enough as to feel that their actions make a difference’ (Petersen, 2020 ). Inculcating ‘optimistic anxiety’ (Tannenbaum et al., 2015 ) is therefore an important feature of crisis communication narratives.
Another important nuance that emerges from Solberg’s posts is her comparisons to other countries to draw attention to the seriousness of the situation. For example, on November 5, 2020, Solberg made the following post announcing new national measures, which received over 5000 likes:
My message to the Norwegian people is: Stay at home as much as possible. Have the least possible social contact with others. It is absolutely necessary to avoid a new shutdown. Norway is at the beginning of the second wave of infection… The virus is spreading rapidly and all counties now have outbreaks. The government is therefore introducing new national infection control measures… If the current rate of infection continues, the number of inpatients in intensive care units will increase sharply in the coming weeks. This will lead to less intensive capacity for other seriously ill people. We are now where the Netherlands was at the beginning of September. A very rapid increase in infection in the Netherlands quickly led to more patients in the intensive care unit… Other European countries have similar experiences. There is therefore a heavy seriousness about the situation. And we must take responsibility together
By giving detailed reasoning behind measures being taken amidst uncertainty, Solberg exhibits both confidence and honesty in her narratives (Lunn et al., 2020 ). Another key feature that emerges from the post above is the emphasis on the risks of an increase in infection, and the possibility of a new lockdown and overburdening of intensive care capacity, thereby reflecting a more strongly persuasive intent. Such emphasis on the risks is different from other posts where Solberg exhibits control and optimism much more strongly. This adaption from a communicative stance to a more persuasive one could result from not only the perceived severity of the situation, but also the perceived risks of pandemic fatigue. Pandemic fatigue has been defined by the WHO as a lack of motivation to adhere to recommended protective behaviours (WHO, 2020b ). According to surveys conducted in different countries, most people have been shown to possess adequate knowledge of COVID-19 and the precautions required to keep safe, yet factors like emotions and context have been found to have greater impact on behaviours than knowledge (Gavi the Vaccine Alliance, 2020 ). A study of different ways of communicating healthcare messages suggested that believability of the messages and the recipients’ reactions to them can be influenced by the persuasive intent (Wang and Shen, 2019 ). Koh et al. ( 2020 ) also discuss the importance of devising effective and successful communications for a sustained period without message fatigue setting in, which includes concern for the way the communication is framed. Overall, we see that Solberg’s posts provide a rationale with portrayal of the government being in control of managing the crisis.
Fostering hope and return to normalcy
Solberg’s posts also emphasized the hopeful aspects of the crisis by appealing to followers to look forward to a return to everyday life, and new educational and economic prospects, despite the difficult current circumstances. This theme aligns with the frame of ‘instilling hope’ as per frame functions for a persuasive narrative by Boin et al. ( 2016 ). During a crisis, more than ever, effective leaders embody the hopes and fears of the society under threat, and therefore they should strive to inculcate optimism of a better future (Boin et al., 2016 ). Previous research has documented that in times of turmoil, followers especially look up to leadership that serves as a beacon of hope for and faith in a positive future, more than they do in times of prosperity (Stam et al., 2018 ; Shamir et al., 1993 ). According to Boin et al., leadership during crisis always has a moral dimension. On January 10, 2021, by which time Norway had witnessed over 50000 cases of infection and over 400 deaths as well as the Gjerdrum disaster, Solberg made the following post:
Dear everyone. This year I hope we can take our dreams back. After a year of pandemic and fear. Then I look forward to seeing creativity unleashed…
Another post that emphasized the optimism for educational prospects was made on April 15, 2020, and drew over 5000 likes:
Today is the last deadline to apply to a vocational school, college or university. I understand that it can feel strange to apply for an education this autumn while the educational institutions keep their campuses closed. Maybe someone also thinks the idea of moving from home to a new city seems extra scary these days. To you I want to say that everyday life will return. Therefore, my appeal to you who want to study: do not put your life on hold, but apply for education this year!
Lessons from previous crises tell us that leaders need to pay attention to the fear of the ongoing threat, as well as sadness and grief, and to provide hope to mitigate social disruption (Maak et al., 2021 ). Here, we see that Solberg’s is attempting to convey hope while also acknowledging the challenges and impact of COVID-19. In doing so, the messages also emphasise self-efficacy and trust in the government. Hope and resilience are closely aligned constructs, as they both include a tendency towards maintaining an optimistic outlook in the face of adversity (Duggal et al., 2016 ). Thus, fostering hope during crisis can help the community cope with the consequences of the crisis. Moreover, by using emotional appeals, leaders can influence attitudes and behaviours as well as induce compassion (Ghio et al., 2020 ).
The theme of fostering hope in Solberg’s posts was found to be particularly emphasized during and before national holidays or important events. Her posts often utilised humour to foster positivity, particularly during critical periods such as during or after implementation of stricter COVID-19 measures. For example, a day after it was announced that infection-reduction measures would continue throughout Christmas, Solberg shared a snipped of her response to a question asked in a press conference and posted:
Can Santa actually come to visit this year?
Creating human moments and hope is a sign of compassionate leadership and helps to establish the relational foundation for widespread support for pandemic control measures (Maak et al., 2021 ). Also, by utilising humour, Solberg adapts the tone of her messages, a tactic that has been found to significantly affect audiences’ attitudes and behaviours, help people manage their emotions, and strengthen support for pandemic measures (Lee and Basnyat, 2013 )
Relating with followers
The last theme is about the posts in which Solberg relates to the public by providing personal information, acknowledging, and relating with the difficult circumstances, and using humour or a private tone in her posts. For example, the post below was made just before Easter and it received more than 13000 likes, making it to be the third-most liked post of Solberg related to COVID-19 during this period.
It will be a different Easter this year. Let’s make the best of it. We can play fun board games with our loved ones, read the book we never have time to read, listen to an audiobook or explore the local area. The last few weeks have been challenging for all of us, but we want to get through this… Sindre and I have recharged with board games and wish you all a very happy Easter!
Empathy is an important component of the persuasive narrative, especially during crises when the decisions made by authorities to mitigate, and control can also have consequences for people’s lives. For crisis communication to be effective, the information provided to the public should not be too factual or portray leaders as distant from the citizens (Shen, 2010 ; Lunn et al., 2020 ). By demonstrating concern and acknowledging the impact of crises, leaders can empathise with the public (Shen, 2010 ; Lunn et al., 2020 ). We see Solberg personifying the challenges of COVID-19 by referring to how the times have been challenging for ‘all of us’. According to Boin et al. ( 2016 ), a leader’s personification of suffering is instrumental in showing empathy because the public is then able to relate to them.
Further, previously in a study by Larsson ( 2015 ) about Norwegian party leaders on Facebook during the 2013 ‘short campaign’, it was found that personal content referencing private life is increasingly employed by Norwegian party leaders. Enli and Rosenberg ( 2018 ) investigated voters’ evaluations of politicians as authentic or ‘real,’ and Solberg was found to be one of the most perceived authentic politicians. Enli ( 2014 ) had earlier suggested that Erna Solberg’s public profile as predictable, anti-elitist and imperfect constructs her authenticity.
A similar example of relatability with followers during the pandemic was the instance when she forgot the rule of not shaking hands during public meetups and press conferences. After the event, she wrote:
It is important that we can have some humour in a difficult time Even a prime minister can forget, but now it is important that we all remember to follow the advice of the health authorities…
She also used an engaging communicative style when interacting with her followers:
Then the holiday is over… a different summer, a little cold, weekly meetings in the Government’s Corona Committee on video, beautiful nature experiences from Norway and a lot of rain. Let me share a wonderful little meeting with a lynx on the lawn on Varaldsøy… Have you had a nice summer?
Thus, Solberg embeds references to her private life, which also helps to personify the messages in her posts and thus relate with the public. In addition, by relating with the public on an everyday basis and through the acknowledgment of shared challenges during crisis, Solberg’s narrative also appears empathetic. Our theme of ‘Relating to the public’ thus encapsulates frame function of ‘showing empathy’ for developing a persuasive narrative, as per Boin et al. ( 2016 ).
Concluding remarks
This paper was an attempt to explore the Facebook posts of Norway’s Prime Minister Erna Solberg to highlight the key features of her crisis communication during the COVID-19 pandemic. By drawing on data from Solberg’s Facebook posts during the pandemic our analyses identified five major themes, (1) Promoting responsibility and togetherness (2) Coping (3) Being in control amidst uncertainty (4) Fostering hope and (5) Relating with the followers, where we went in detail explanation by using frame functions of a persuasive narrative by Boin et al. ( 2016 ). We furthermore discussed the specific Norwegian contextual nuances to the frame functions. These were the theme ‘Responsibilization and togetherness’, presented via the references to Norwegianness and the cultural concept and practice of dugnad . Hence, our paper showed how during crisis persuasive narratives are incorporated into the social media communication strategies of political leaders.
The paper also showed how persuasive narratives are delivered through praising the public’s efforts, promoting togetherness, caring about the public’s well-being, displaying optimism and confidence in the government’s measures. It elaborated on how crisis management on social media was done via the use of humour and personal information. Humour was used as a tool to engage with the public and help them relate and comply to the COVID-19 restrictions. Hence, Solberg used Facebook to capitalise on a wide-reaching social medium (Hallahan, 2010 ). While the communication of leaders during crises helps to fill the cognitive void, the use of social media helps build societal resilience by improving awareness and encouraging preparedness (Boin et al., 2016 )
Even so, the success of a persuasive narrative is to a great extent dependant on the credibility of its proponents (Boin et al., 2016 ). The reputation of the leader and the organisation that they represent plays a key role in framing a successful persuasive narrative. In general, Norwegians have more trust in each other and their institutions than most other countries (Skirbekk and Grimen, 2012 ). A survey conducted by the Norwegian Citizen’s Panel [Norsk Medborgerpanel] in March 2020 found that trust in government, in the health authorities, in parliament, and in national and local politicians had increased, as did trust in the Prime Minister during the pandemic (Dahl, 2020 ). Clearly, Solberg seems to have benefitted from the trust capital in Norwegian society with her Facebook communications during a crisis. More recently, Erna Solberg has received heavy criticism for breach of COVID-19 restrictions during a family trip to Geilo for her 60th birthday (The Guardian, 2021a ). Following which, Erna Solberg, has been investigated by police and fined (The Guardian, 2021b ). Thus, while her Facebook posts exhibiting components of a persuasive narrative received popularity, her actions have nevertheless been subjected to scrutiny and criticisms in mainstream media (Larsen, 2021 ). According to Boin et al. ( 2016 : p. 72), the retainment of confidence of the public is essential for the communication strategies to be effective. Therefore, such media criticism might undermine the credibility of Solberg and her cabinet, leading to less credible and politically ineffective narratives. On the other hand, past performances, and reputation also play an important role in increasing leaders’ personal credibility in the face of crisis (Boin et al., 2016 ). Consequently, Solberg’s long career in politics and her reputation of caring about the citizens as previously discussed, could buffer the recent impact on her credibility. Moreover, communication during and after a crisis affects long-term impressions (Coombs, 2007 ). With the personification of politics in Norway or ‘decentralising personalization’ (Balmas et al., 2014 ), the criticisms paved at Erna, however, reflect more of a personal crisis than a national crisis. And while we do not analyse Solberg’s posts beyond 9 th Feb. 2021 i.e., after Solberg spoke about the Geilo trip incident on her Facebook account, we see that she follows similar strategy in handling this personal crisis as the national crisis of COVID-19, through use of a persuasive narrative. Future studies can therefore focus on how Solberg and other political leaders utilise the strategy of persuasive narrative in management of personal crisis in nexus with national crisis such as that of COVID-19.
Further, we concur with Christensen and Lægreid ( 2020 ) who write that the ‘political leadership has succeeded well in connecting governance capacity and legitimacy using the argument that Norway had sufficient resources to deal with the crisis. While the health resource capacity and preparedness of Norway inarguably contributes to the outcomes of the crisis, communicating a successful persuasive narrative with credibility is integral to gaining legitimacy and filling the cognitive void (Boin et al., 2016 ). Erna Solberg’s use of persuasive narrative in Facebook posts, seems therefore to have been effective in the management of the COVID-19 pandemic, but her latest unfortunate incident goes to show how politicians’ management of crises is tenuous and highly dependent on public trust.
Our study adds to the significance and knowledge of how persuasive narratives are incorporated into the communication strategy of leaders on a social media platform and highlights the usefulness of this framework for studies about ongoing and future crises. By using data from social media, our findings also add to the understanding of the increased personification of politics and how leaders utilise this personification to communicate government measures and engage with the public during a crisis. Future research can further explore how public leaders and health authorities’ frame crises situations, actions, issues, and responsibility to dramatise and reinforce key ideas (Hallahan, 1999 ). Such insights can pave way for understanding public’s shaping of risk perceptions and compliance to behavioural measures during crises such as the COVID-19 pandemic.
Data availability
The dataset analysed during the current study is available through the public profile of Erna Solberg on Facebook: https://www.facebook.com/ernasolberg/ . This dataset was derived from Crowd Tangle which can be accessed through request at https://www.crowdtangle.com/ .
Known as ‘hyttetur’, cabin trips are deeply rooted in Norwegian culture and way of life
Crowdtangle extracts both historical and current data of post contents and metadata such as the date the post was made, number of likes, other reactions and shares. Information about how to access raw material included in this study can be found in the data availability statement at the end of the article.
‘Everything will be fine’ [ Alt blir bra ] was one of the campaigns that spread because of the COVID-19 crisis in Norway depicting pictures of a rainbow.
Aldoory L (2010) The ecological perspective and other ways to (re)consider cultural factors in risk communication. In: Heath R, O’ Hair (eds) Handbook of risk and crisis communication. Routledge, New York, pp. 227–246
Google Scholar
Balmas M, Rahat G, Sheafer T, Shenhav SR (2014) Two routes to personalized politics: Centralized and decentralized personalization. Party Polit 20(1):37–51. https://doi.org/10.1177/1354068811436037
Article Google Scholar
Blix I, Birkeland MS, Thoresen S (2021) Worry and Mental Health in the COVID-19 Pandemic: Vulnerability Factors in the General Norwegian Population. https://doi.org/10.21203/rs.3.rs-192098/v1 . Accessed 10 Jun 2021
Boin A, Stern E, Sundelius B (2016) The politics of crisis management: Public leadership under pressure. Cambridge University Press
Boudreau MC, Gefen D, Straub DW (2001) Validation in information systems research: a state-of-the-art assessment. MIS Quart 25(1):1. https://doi.org/10.2307/3250956
Brandt P, Wörlein J (2020) Government crisis communication during the pandemic. https://www.sciencespo.fr/en/news/news/government-crisis-communications-during-the-pandemic/4862 . Accessed 20 May 2021
Braun V, Clarke V (2006) Using thematic analysis in psychology. Qual Res Psychol 3(2):77–101. https://doi.org/10.1191/1478088706qp063oa
Brassey J, Kruyt M (2020) How to demonstrate calm and optimism in a crisis. McKinsey & Company, April. 2020. https://www.mckinsey.com/business-functions/organization/our-insights/how-to-demonstrate-calm-and-optimism-in-a-crisis . Accessed 27 May 2021
Brügger N (2013) Historical network analysis of the web. Soc Sci Comput Review 31(3):306–21. https://doi.org/10.1177/0894439312454267
Christensen T, Lægreid P (2020) Balancing governance capacity and legitimacy: how the Norwegian government handled the COVID‐19 crisis as a high performer. Public Admin Rev 80(5):774–9. https://doi.org/10.1111/puar.13241
Collins M, Neville K, Hynes W, Madden M (2016) Communication in a disaster-the development of a crisis communication tool within the S-HELP project. J Decis Syst 25(1):160–170. https://doi.org/10.1080/12460125.2016.1187392
Coombs WT (2007) Protecting organization reputations during a crisis: the development and application of situational crisis communication theory. Corp Reput Rev 10(3):163–176. https://doi.org/10.1057/palgrave.crr.1550049
Coombs WT (2015) Ongoing crisis communication: planning, managing and responding. Sage, Thousand Oaks, CA
CrowdTangle (2021) CrowdTangle Team. Facebook, Menlo Park, California, United States. List ID: 1504404 2021
Dada S, Ashworth HC, Bewa MJ, Dhatt R (2021) Words matter: political and gender analysis of speeches made by heads of government during the COVID-19 pandemic. BMJ Global Health 6(1):e003910. https://doi.org/10.1101/2020.09.10.20187427
Article CAS PubMed Google Scholar
Dagsavisen (2020) FHI: Norge ble varslet om koronasmitte fra Østerrike allerede 4. mars 2020 (Norway was notified of corona infection from Austria as early as 4 March 2020). https://www.dagsavisen.no/nyheter/innenriks/2020/10/30/fhi-norge-ble-varslet-om-koronasmitte-fra-osterrike-allerede-4-mars/ . Accessed on 1 Apr 2021
Dahl T (2020) Stolar meir på Erna og mindre på naboen (Rely more on Erna and less on the neighbor). https://www.uib.no/aktuelt/135017/stolar-meir-p%C3%A5-erna-og-mindre-p%C3%A5-naboen . Accessed 3 Jul 2021
Davies B, Harré R (1990) Positioning: the discursive production of selves. J Theory Soc Behav 20(1):43–63. https://doi.org/10.1111/j.1468-5914.1990.tb00174.x
Duggal D, Sacks-Zimmerman A, Liberta T (2016) The impact of hope and resilience on multiple factors in neurosurgical patients. Cureus 8(10). https://doi.org/10.7759/cureus.849
Enli G (2014) Mediated authenticity. Peter Lang Incorporated, New York
Enli G, Rosenberg LT (2018) Trust in the age of social media: Populist politicians seem more authentic. Soc Media Soc 4(1):2056305118764430. https://doi.org/10.1177/2056305118764430
Eriksen TH (2020) Norway’s response to Covid-19 and the Janus face of Nordic trust. https://www.coronatimes.net/norway-covid-19-nordic-trust/ . Accessed on 15 May 2021
Finset A, Bosworth H, Butow P, Gulbrandsen P, Hulsman RL, Pieterse AH et al. (2020) Effective health communication–a key factor in fighting the COVID-19 pandemic. Patient Educ Couns 103(5):873. https://doi.org/10.1016/j.pec.2020.03.027
Article PubMed PubMed Central Google Scholar
Gavi the Vaccine Alliance (2020) 10 reasons why pandemic fatigue could threaten global health in 2021. https://www.gavi.org/vaccineswork/10-reasons-why-pandemic-fatigue-could-threaten-global-health-2021 . Accessed 15 Jun 2021
Ghio D, Lawes-Wickwar S, Tang M, Epton T, Howlett N, Jenkinson E (2020) What influences people’s responses to public health messages for managing risks and preventing infectious diseases? A rapid systematic review of the evidence and recommendations. https://doi.org/10.31234/osf.io/nz7tr . Accessed 28 May 2021
Golbeck J, Grimes JM, Rogers A (2010) Twitter use by the US Congress. J Am Soc Inform Sci Technol 61(8):1612–21. https://doi.org/10.1002/asi.21344
Gruber DA, Smerek RE, Thomas-Hunt MC, James EH (2015) The real-time power of Twitter: Crisis management and leadership in an age of social media. Bus Horizon 58(2):163–172. https://doi.org/10.1016/j.bushor.2014.10.006
Hallahan K (1999) Seven models of framing: implications for public relations. J Public Relat Res 11(3):205–242. https://doi.org/10.1207/s1532754xjprr1103_02
Hallahan K (2010) Crises and risk in cyberspace. In: Heath R, Hair O’ (ed) Handbook of risk and crisis communication. Routledge, New York, NY, pp. 412–445
Han RH, Schmidt MN, Waits WM, Bell AK, Miller TL (2020) Planning for mental health needs during COVID-19. Curr Psychiatry Rep 22(12):1–10. https://doi.org/10.1007/s11920-020-01189-6
Heath R, O’ Hair H (2010) The significance of crisis and risk communication. In: Heath R, Hair O’ (ed) Handbook of risk and crisis communication. Routledge, New York, pp. 5–30
Chapter Google Scholar
Henderson B, Vikander N (eds) (2007) Nature first: outdoor life the friluftsliv way. Dundurn
Houston JB et al. (2014) Social media and disasters: a functional framework for social media use in disaster planning, response, and research. Disasters 39(1):1–22. https://doi.org/10.1111/disa.12092
Article PubMed Google Scholar
Hungnes S (2016) Den norske dugnadskulturen (The Norwegian voluntary culture. https://agendamagasin.no/kommentarer/den-norske-dugnadskulturen/ . Accessed 25 May 2021
Jenzen O, Erhart I, Eslen-Ziya H, Korkut U, McGarry A (2021) The symbol of social media in contemporary protest: Twitter and the Gezi Park movement. Convergence 27(2):414–37. https://doi.org/10.1177/1354856520933747
Jørgensen-Vittersø KA (2021) From fresh air and sunbathing to wildlife and snow caves: ‘Friluftsliv’in norwegian primary schools, 1939–1980. In: Roos M, Berge KL, Edgren H (eds) Exploring textbooks and cultural change in nordic education 1536–2020. Brill, pp 245–259
Karlsen R, Enjolras B (2016) Styles of social media campaigning and influence in a hybrid political communication system: linking candidate survey data with Twitter data. Inte J Press/Politics 21(3):338–57. https://doi.org/10.1177/1940161216645335
Kavanaugh AL, Fox EA, Sheetz SD, Yang S, Li LT, Shoemaker DJ et al. (2012) Social media use by government: from the routine to the critical. Gov Inform Q 29(4):480–91. https://doi.org/10.1145/2037556.2037574
Kim S, Liu BF (2012) Are all crises opportunities? A comparison of how corporate and government organizations responded to the 2009 flu pandemic. J Public Relat Res 24(1):69–85. https://doi.org/10.1080/1062726x.2012.626136
Koh PK-K, Chan LL, Tan E-K (2020) Messaging fatigue and desensitisation to information during pandemic. Arch Med Res 51(7):716–717. https://doi.org/10.1016/j.arcmed.2020.06.014
Article CAS PubMed PubMed Central Google Scholar
Larsen K (2021) Erna Solbergs popularitet stuper (Erna Solberg’s popularity plummets). https://www.dagbladet.no/nyheter/erna-solbergs-popularitet-stuper/73597485 . Accessed 15th Apr
Larsson AO (2015) Pandering, protesting, engaging. Norwegian party leaders on Facebook during the 2013 ‘Short campaign’. Inform Commun Soc 18(4):459–73. https://doi.org/10.1080/1369118x.2014.967269
Lee ST, Basnyat I (2013) From press release to news: mapping the framing of the 2009 H1N1 A influenza pandemic. Health Commun 28(2):119–32. https://doi.org/10.1080/10410236.2012.658550
Lund J (2021) Somling, rot og ulovligheter (Procrastination, clutter and illegalities). https://www.aftenposten.no/meninger/kommentar/i/BlPRjw/somling-rot-og-ulovligheter . Accessed on 25 May 2021
Lunn P, Belton C, Lavin C, McGowan F, Timmons S, Robertson D (2020) Using behavioural science to help fight the coronavirus. J Behav Public Administration, 3(1). https://doi.org/10.30636/jbpa.31.147
Maak T, Pless NM, Wohlgezogen F (2021) The fault lines of leadership: Lessons from the global Covid-19 crisis. J Change Manag 21(1):66–86. https://doi.org/10.1080/14697017.2021.1861724
Moss SM, Sandbakken EM (2021) “Everybody needs to do their part, so we can get this under control.” reactions to the norwegian government meta‐narratives on COVID‐19 measures. Polit Psychol 42(5):881–898. https://doi.org/10.1111/pops.12727
Notaker H, Tvedt KA (2021) Stor Norske Leksikon: Erna Solberg ( https://snl.no/Erna_Solberg . Accessed on 20 Apr 2021
Nilsen ACE, Skarpenes O (2020) Coping with COVID-19. Dugnad: a case of the moral premise of the Norwegian welfare state. International Journal of Sociology and Social Policy. (ahead-of-print). https://doi.org/10.1108/ijssp-07-2020-0263
Petersen MB (2020) The unpleasant truth is the best protection against coronavirus. Politiken. https://pure.au.dk/portal/files/181464339/The_unpleasant_truth_is_the_best_protection_against_coronavirus_Michael_Bang_Petersen.pdf . Accessed 11 Jun 2021
Reddy BV, Gupta A (2020) Importance of effective communication during COVID-19 infodemic. J Fam Med Prim Care 9(8):3793. https://doi.org/10.4103/jfmpc.jfmpc_719_20
Reuters (2013) Iron Erna’s softer side wins through in Norway election 2013. https://www.scmp.com/news/world/article/1307898/iron-ernas-softer-side-wins-through-norway-election . Accessed 27 Apr 2021
Sandelowski M (1994) Focus on qualitative methods. The use of quotes in qualitative research. Res Nurs Health 17(6):479–482. https://doi.org/10.1002/nur.4770170611
Sang X, Menhas R, Saqib ZA, Mahmood S, Weng Y, Khurshid S, et al. (2020) The psychological impacts of CoViD-19 home confinement and physical activity: a structural equation model analysis. Front Psychol 11. https://doi.org/10.3389/fpsyg.2020.614770
Schultz F, Utz S, Göritz A (2011) Is the medium the message? Perceptions of and reactions to crisis communication via twitter, blogs and traditional media. Public Relat Rev 37(1):20–27. https://doi.org/10.1016/j.pubrev.2010.12.001
Shah K, Kamrai D, Mekala H, Mann B, Desai K, Patel RS (2020) Focus on mental health during the coronavirus (COVID-19) pandemic: applying learnings from the past outbreaks. Cureus 12(3). https://doi.org/10.7759/cureus.7405
Shamir B, House RJ, Arthur MB (1993) The motivational effects of charismatic leadership: a self-concept based theory. Organ Sci 4(4):577–94. https://doi.org/10.1287/orsc.4.4.577
Shen L (2010) Mitigating psychological reactance: the role of message-induced empathy in persuasion. Hum Commun Res 36(3):397–422. https://doi.org/10.1111/j.1468-2958.2010.01381.x
Article ADS Google Scholar
Simon C, Mobekk H (2019) Dugnad: a fact and a narrative of Norwegian prosocial behavior. Perspect Behav Sci 42(4):815–34. https://doi.org/10.1007/s40614-019-00227-w
Skirbekk H, Grimen H (2012) Tillit i Norge (Trust in Norway). Res Publica, Oslo
Stam D, van Knippenberg D, Wisse B, Nederveen Pieterse A (2018) Motivation in words: promotion-and prevention-oriented leader communication in times of crisis. J Manag 44(7):2859–87. https://doi.org/10.1177/0149206316654543
Stephens KK, Barrett AK, Mahometa MJ (2013) Organizational communication in emergencies: Using multiple channels and sources to combat noise and capture attention. Hum Commun Res 39(2):230–251. https://doi.org/10.1111/hcre.12002
Sutton J, Spiro E, Butts C, Fitzhugh S, Johnson B, Greczek M (2013) Tweeting the spill: Online informal communications, social networks, and conversational microstructures during the Deepwater Horizon oilspill. Int J Inform Syst Crisis Resp Manag 5(1):58–76. https://doi.org/10.4018/jiscrm.2013010104
Tannenbaum MB, Hepler J, Zimmerman RS, Saul L, Jacobs S, Wilson K et al. (2015) Appealing to fear: a meta-analysis of fear appeal effectiveness and theories. Psychol Bull 141(6):1178. https://doi.org/10.1037/a0039729
The Guardian (2021a) Norwegian PM Erna Solberg investigated for Covid rules breach. Available at: https://www.theguardian.com/world/2021/mar/19/norwegian-pm-erna-solberg-investigated-for-covid-rules-breach . Accessed 25th Mar 2021
The Guardian (2021b) Norwegian PM fined after breaking Covid rules with birthday party. Available at: https://www.theguardian.com/world/2021/apr/09/norway-prime-minister-erna-solberg-fined-breaking-covid-rules-birthday . Accessed 15th Mar 2021
Tjora A (2020) Tillitsfull dugnad eller instruert solidaritet (Trusting voluntary work or instructed solidarity) https://www.universitetsavisa.no/koronavirus-ytring/tillitsfull-dugnad-eller-instruert-solidaritet/111642 . Accessed on 21 May 2021
Utz S, Schultz F, Glocka S (2013) Crisis communication online: How medium, crisis type and emotions affected public reactions in the Fukushima Daiichi nuclear disaster. Public Relat Rev 39(1):40–46. https://doi.org/10.1016/j.pubrev.2012.09.010
Van Dijck J (2013) Facebook and the engineering of connectivity: A multi-layered approach to social media platforms. Convergence 19(2):141–55. https://doi.org/10.1177/1354856512457548
Vogt H, Pahle A (2020) En fryktdrevet pandemi av varige helseproblemer (A fear-driven pandemic of lasting health problems) https://www.aftenposten.no/meninger/kronikk/i/opdB6a/en-fryktdrevet-pandemi-av-varige-helseproblemer . Accessed 20 May 2021
Wang W, Shen F (2019) The effects of health narratives: Examining the moderating role of persuasive intent. Health Market Q 36(2):120–35. https://doi.org/10.1080/07359683.2019.1575061
Article MathSciNet Google Scholar
Werliin R, Kokholm M (2016) Device study: Social media across the Nordics. https://www.audienceproject.com/wp-content/uploads/study_social_media_across_the_nordics.pdf . Accessed 18 Jun 2021
World Health Organization (2020a) Mental health and psychosocial considerations during the COVID-19 outbreak, 18 March 2020. https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf . Accessed 10 Jun 2021
World Health Organization (2020b) Pandemic fatigue: reinvigorating the public to prevent COVID-19: policy framework for supporting pandemic prevention and management: revised version November 2020. World Health Organization. Regional Office for Europe. https://apps.who.int/iris/handle/10665/337574 . Accessed 17 Jun 2021
World Health Organization (2021) WHO Coronavirus (COVID-19) Dashboard 2021 https://covid19.who.int/?gclid=Cj0KCQjw9_mDBhCGARIsAN3PaFNVuA3kABELXjY66cXUIVcTNNBkPrX57w1OtZL1GYBomSnvTRflQTcaAoxkEALw_wcB . Accessed 18 Apr 2021
Download references
Acknowledgements
This article is published as part of the research project ‘Fighting Pandemics with Enhanced Risk Communication: Messages, Compliance and Vulnerability During the COVID-19 Outbreak (PAN-FIGHT)’, which is financed by the Norwegian Research Council (Project number: 312767).
Author information
Authors and affiliations.
University of Stavanger, Stavanger, Norway
Sanjana Arora & Hande Eslen-Ziya
Oslo Metropolitan University, Oslo, Norway
Jonas Debesay
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Sanjana Arora .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors.
Informed consent
Additional information.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Arora, S., Debesay, J. & Eslen-Ziya, H. Persuasive narrative during the COVID-19 pandemic: Norwegian Prime Minister Erna Solberg’s posts on Facebook. Humanit Soc Sci Commun 9 , 35 (2022). https://doi.org/10.1057/s41599-022-01051-5
Download citation
Received : 12 October 2021
Accepted : 17 January 2022
Published : 01 February 2022
DOI : https://doi.org/10.1057/s41599-022-01051-5
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
This article is cited by
Norwegian “dugnad” as a rhetorical device in public health communication during the covid-19 pandemic. a qualitative study from immigrant’s perspectives.
- Raquel Herrero-Arias
- Irina Vladimirovna Halbostad
- Esperanza Diaz
Archives of Public Health (2024)
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies


An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Elsevier - PMC COVID-19 Collection
Examining persuasive message type to encourage staying at home during the COVID-19 pandemic and social lockdown: A randomized controlled study in Japan
- • We examined persuasive message types in terms of a narrator encouraging self-restraint.
- • Messages from a governor, an expert, a physician, a patient, and a resident were compared.
- • The message from a physician increased intention to stay at home the most.
- • The physician’s message conveyed the crisis of collapse of the medical system.
Behavioral change is the only prevention against the COVID-19 pandemic until vaccines become available. This is the first study to examine the most persuasive message type in terms of narrator difference in encouraging people to stay at home during the COVID-19 pandemic and social lockdown.
Participants (n = 1,980) were randomly assigned to five intervention messages (from a governor, a public health expert, a physician, a patient, and a resident of an outbreak area) and a control message. Intention to stay at home before and after reading messages was assessed. A one-way ANOVA with Tukey’s or Games–Howell test was conducted.
Compared with other messages, the message from a physician significantly increased participants’ intention to stay at home in areas with high numbers of people infected (versus a governor, p = .002; an expert, p = .023; a resident, p = .004).
The message from a physician―which conveyed the crisis of overwhelmed hospitals and consequent risk of people being unable to receive treatment―increased the intent to stay at home the most.
Practice implications
Health professionals and media operatives may be able to encourage people to stay at home by disseminating the physicians’ messages through media and the internet.
1. Introduction
The outbreak of the coronavirus disease 2019 (COVID-19) has emerged as the largest global pandemic ever experienced [ 1 ]. Experts have proposed that social lockdown will lead to improvements such as controlling the increase in the number of infected individuals and preventing a huge burden on the healthcare system [ [2] , [3] , [4] ]. Governments of many countries across the world have declared local and national social lockdown [ 4 , 5 ]. In April 2020, the Japanese government declared a state of emergency, which allows prefectural governors to request residents to refrain from unnecessary and nonurgent outings from home [ 6 ]. However, despite such governor declarations, people in various countries have resisted and disregarded calls to stay at home [ [7] , [8] , [9] ]. Because social lockdown is the only existing weapon for prevention of the pandemic until vaccines becomes available to treat COVID-19, behavioral change in individuals regarding staying at home is crucial [ 3 , 4 ]. Many news articles about COVID-19 are published daily by the mass media and over the internet. Such articles convey messages from governors, public health experts, physicians, COVID-19 patients, and residents of outbreak areas, encouraging people to stay at home. This is the first study to examine which narrator’s message is most persuasive in encouraging people to do so during the COVID-19 pandemic and social lockdown.
2.1. Participants and design
Participants were recruited from people registered in a survey company database in Japan. The eligibility criterion was men and women aged 18–69 years. Exclusion criteria were individuals who answered screening questions by stating: that they cannot go out because of illness or disability; that they have been diagnosed with a mental illness; or/and that they or their family members have been infected with COVID-19. A total of 1,980 participants completed the survey from May 9–11, 2020, when the state of emergency covered all prefectures in Japan. Participants were included according to the population composition ratio in Japan nationwide by gender, age, and residential area. Participants were randomly assigned either to a group that received an intervention message (i.e., from a governor, a public health expert, a physician, a patient, and a resident of the outbreak area) or to one that received a control message. The study was registered as a University Hospital Medical Information Network Clinical Trials Registry (number: UMIN000040286) on May 1, 2020. The methods of the present study adhered to CONSORT guidelines. The protocol was approved by the ethical review committee at the Graduate School of Medicine, University of Tokyo (number: 2020032NI). All participants gave written informed consent in accordance with the Declaration of Helsinki.
2.2. Intervention and control messages
We searched news articles about COVID-19 using Yahoo! JAPAN News ( https://news.yahoo.co.jp ), the largest Japanese news portal site. We also searched videos posted by residents of outbreak areas such as New York using YouTube ( https://www.youtube.com/user/YouTubeJapan ). By referring to these articles and videos, we created five intervention messages from a governor, a public health expert, a physician, a patient, and a resident of an outbreak area. The content of each message encouraged readers to stay at home. We included threat and coping messages in each intervention message based on protection motivation theory (PMT) [ 10 , 11 ]. Appendix A shows the five intervention messages used in this study, translated into English for this report. For a control message we obtained textual information about bruxism from the website of the Ministry of Health, Labour and Welfare ( https://www.e-healthnet.mhlw.go.jp/ ).
2.3. Measures
The primary outcome was intention to stay at home. The secondary outcomes were PMT constructs (i.e., perceived severity, vulnerability, response efficacy, and self-efficacy). Participants responded to two or three questions for each measure (see Appendix B ). These measures were adapted and modified from previous studies [ [12] , [13] , [14] , [15] ]. All primary and secondary outcomes were measured before and after the participants read intervention or control messages, and mean scores were calculated. Higher scores indicated greater intention and perception. All participants were asked for their sociodemographic information before they read intervention or control messages.
2.4. Sample size
Based on the effect size in a previous randomized controlled study [ 16 ], we estimated a small effect size (Cohen’s d = .20) in the current study. We conducted a power analysis at an alpha error rate of .05 (two-tailed) and a beta error rate of .20. The power analysis indicated that 330 participants were required in each of the intervention and control groups.
2.5. Statistical analysis
A one-way analysis of variance (ANOVA) was conducted with the absolute change in mean values for each measure before and after intervention as the dependent variable and the group assignment as the independent variable. For multiple comparisons, Tukey’s test was conducted on significant main effects where appropriate. The Games–Howell test was performed when the assumption of homogeneity of variances was not satisfied. Additionally, we conducted subgroup analyses including only participants who lived in 13 “specified warning prefectures,” where the number of infected individuals showed a marked increase [ 17 ]. A p value of <.05 was considered significant in all statistical tests. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 21.0 (IBM, Armonk, NY, USA).
Table 1 shows the participants’ characteristics. Table 2 , Table 3 present a comparison among the five intervention groups using one-way ANOVA and multiple comparisons when including all prefectures and only participants who lived in the specified warning prefectures, respectively. More significant differences between intervention messages were found in the specified warning prefectures compared with all prefectures. In Table 3 , the Games–Howell test indicates that the message from a physician increased participants’ intention to stay at home significantly more than other narrators’ messages (versus a governor, p = .002; an expert, p = .023; a resident, p = .004). Multiple comparisons demonstrated that the message from a physician increased participants’ perceived severity (versus a governor, p = .015), response efficacy (versus a resident, p = .014), and self-efficacy (versus a governor, p = .022; a patient, p = .009) significantly more than other narrators’ messages.
Participants’ sociodemographic information.
Comparison of amount of change before and after intervention among groups when including all prefectures (N = 1,980).
Comparison of amount of change before and after intervention among groups when including only the “specified warning prefectures” (N = 1,274).
4. Discussion and conclusion
4.1. discussion.
As Appendix A shows, the message from a physician specifically communicated the critical situation of hospitals being overwhelmed and the consequent risk of people being unable to receive treatment. Depiction of the crisis of overwhelmed hospitals may have evoked heightened sensation that elicited sensory, affective, and arousal responses in recipients. Social lockdown presumably evoked psychological reactance in many individuals [ 18 ]. Psychological reactance is considered one of the factors that impedes individuals’ staying at home during a pandemic [ 18 ]. Studies of psychological reactance have indicated that heightened sensation is the feature of a message that reduces psychological reactance [ 19 , 20 ]. Additionally, in Japan recommendations by physicians have a strong influence on individuals’ decision making owing to the remnants of paternalism in the patient–physician relationship [ 21 ]. These may constitute the reasons for the message from a physician generating the greatest impact on recipients’ protection motivation.
Public health professionals, governors, media professionals, and other influencers should use messages from physicians and disseminate relevant articles through the media and social networking services to encourage people to stay at home. It is important that health professionals and media have a network and collaborate with one another [ 22 ]. To build relationships and provide reliable resources, health professionals are expected to hold press conferences and study meetings with journalists. Through such networking, journalists can acquire accurate information in dealing with the pandemic, such as using messages from physicians to encourage people to stay at home. Consequently, journalists should disseminate such messages. It is also important that governments, municipalities, medical associations, and other public institutions convey messages from physicians and that the media effectively spread those messages. Owing to the advances of Web 2.0 [ 23 ], health professionals’ grassroots communication with journalists and citizens via social media may provide opportunities for many people to access persuasive messages from physicians.
4.1.1. Limitations
First, the content of the intervention messages in this study may not represent voices of all governors, public health experts, physicians, patients, and residents of outbreak areas. Second, it is not clear from this study which sentences in the intervention message made the most impact on recipients and why. Third, this study assessed intention rather than actual behavior. Finally, it is unclear as to what extent the present findings are generalizable to populations other than the Japanese participants in this study.
4.2. Conclusion
In areas with high numbers of infected people, the message from a physician, which conveyed the crisis of hospitals being overwhelmed and the consequent risk of people being unable to receive treatment, increased the intention to stay at home to a greater extent than other messages from a governor, a public health expert, a patient with COVID-19, and a resident of an outbreak area.
4.3. Practice implications
Governors, health professionals, and media professionals may be able to encourage people to stay at home by disseminating the physicians’ messages through media such as television and newspapers as well as social networking services on the internet.
This work was supported by the Japan Society for the Promotion of Science KAKENHI (grant number 19K10615).
CRediT authorship contribution statement
Tsuyoshi Okuhara: Conceptualization, Methodology, Formal analysis, Investigation, Writing - original draft, Funding acquisition. Hiroko Okada: Methodology, Investigation, Writing - review & editing. Takahiro Kiuchi: Supervision, Writing - review & editing.
Declaration of Competing Interest
The authors declare that there is no conflict of interest.
Acknowledgement
We thank Hugh McGonigle, from Edanz Group ( https://en-author-services.edanzgroup.com/ac ), for editing a draft of the manuscript.
Appendix A.
Intervention: the message from a governor.
The following is a message from the governor of your local area.
Please avoid leaving your house as much as possible.
Staying at home can save lives and prevent the spread of infection.
Intervention: The message from an expert
The following is a message from an infectious disease control expert.
Intervention: The message from a physician
The following is a message from an emergency medical care doctor.
Intervention: The message from a patient
The following is a message from a patient who is infected with the novel coronavirus.
Intervention: The message from a resident
The following is a message from an individual who lives in an area where an outbreak of novel coronavirus has occurred.
A control message
According to the traditional definition, grinding one’s teeth is when somebody makes a sound by strongly grinding the teeth together, usually unconsciously or while asleep. Nowadays, it is often referred to as ‘teeth grinding,’ a term which also covers various actions that we do while awake.
Whether you are sleeping or awake, the non-functional biting habit of grinding one’s teeth dynamically or statically, or clenching one’s teeth, can also be referred to as bruxism (sleep bruxism if it occurs at night). Bruxism can be categorized into the movements of: sliding the upper and lower teeth together like mortar and pestle (grinding); firmly and statically engaging the upper and lower teeth (clenching); and dynamically bringing the upper and lower teeth together with a tap (tapping).
Bruxism is difficult to diagnose, as it often has no noticeable symptoms. Stress and dentition are thought to be causes of bruxism, but it is currently unclear and future research is anticipated.
Splint therapy, which involves the use of a mouthpiece as an artificial plastic covering on one’s teeth, and cognitive behavioral therapy are being researched as treatments for bruxism.
Appendix B.
All questions above were on a scale of 1–6, ranging from “extremely unlikely” to “unlikely,” “a little unlikely,” “a little likely,” “likely,” and “extremely likely.”
- Ethics & Leadership
- Fact-Checking
- Media Literacy
- The Craig Newmark Center
- Reporting & Editing
- Ethics & Trust
- Tech & Tools
- Business & Work
- Educators & Students
- Training Catalog
- Custom Teaching
- For ACES Members
- All Categories
- Broadcast & Visual Journalism
- Fact-Checking & Media Literacy
- In-newsroom
- Memphis, Tenn.
- Minneapolis, Minn.
- St. Petersburg, Fla.
- Washington, D.C.
- Poynter ACES Introductory Certificate in Editing
- Poynter ACES Intermediate Certificate in Editing
- Ethics & Trust Articles
- Get Ethics Advice
- Fact-Checking Articles
- International Fact-Checking Day
- Teen Fact-Checking Network
- International
- Media Literacy Training
- MediaWise Resources
- Ambassadors
- MediaWise in the News
Support responsible news and fact-based information today!
The World Health Organization’s pandemic plan won’t end free speech
A draft of the who’s pandemic accord says that the document will be used with respect to individual’s personal freedoms.

As the world emerged from a global pandemic, the World Health Organization began drafting a legal agreement to respond to future pandemics. Since then, the document has been a target of misinformation.
The WHO’s pandemic prevention, preparedness and response accord is a legal agreement the organization’s 194 member states, including the U.S., are negotiating to help prevent and better prepare for future pandemics.
In a clip from former Fox News anchor Tucker Carlson’s web show, author Bret Weinstein warned the WHO’s actions with regard to the accord could strip Americans of their constitutionally protected rights to free speech.
“So, you’re saying that an international health organization could just end the First Amendment?” Carlson asked Weinstein in the clip, which circulated Jan. 28 in an Instagram video and was attracting comments and interactions in late April.
“The ability to do it is currently under discussion at the international level,” replied Weinstein, whose COVID-19 claims PolitiFact has previously fact – checked.
The Instagram post was flagged as part of Meta’s efforts to combat false news and misinformation on its News Feed. (Read more about our partnership with Meta , which owns Facebook and Instagram.)
The clip came from a video published Jan. 5 on the subscription-based Tucker Carlson Network website. The network also shared a longer clip of this portion of the video on its YouTube page .
The longer version shows a fuller exchange:
Carlson: “So, you’re saying that an international health organization could just end the First Amendment?” Weinstein: “Yes, and I know it sounds preposterous — ” Carlson: “It does not sound preposterous.” Weinstein: “The ability to do it is currently under discussion at the international level.” Weinstein later said the WHO’s pandemic preparedness plan will be used to silence podcasters and eliminate “ national and personal sovereignty .”
Weinstein did not respond to PolitiFact’s request for comment.
But his assertion that the WHO’s work on this plan could eliminate Americans’ free speech protections is contradicted by the U.S. Constitution and the draft accord itself.
A March 28 WHO press release said the pandemic agreement’s draft will continue to be refined ahead of the World Health Assembly , set for May 27 to June 1 in Geneva, Switzerland.
An April draft of the plan explicitly stated that the plan’s implementation will be with “full respect for the dignity, human rights and fundamental freedoms of persons” and that states have the sovereign right” to “adopt, legislate and implement legislation.”
World Health Organization information also details that the governments themselves would determine the accord, with member states deciding the terms.
Lawrence Gostin, director of Georgetown University’s O’Neill Institute for National and Global Health Law, told PolitiFact that the pandemic accord contains no provision that would override any U.S. law.
“The Pandemic Agreement would not control what could or could not be written or said in the United States,” Gostin said. “The regulation of speech, including online content, is entirely within the realm of the US Congress.” He added that there is a domestic process for amending the constitution.
The process of changing the U.S. Constitution is lengthy . To eliminate the First Amendment, Congress would have to propose the change with a majority vote in both the House of Representatives and the Senate. An amendment can also be proposed during a constitutional convention called for by two-thirds of the state legislatures . For the amendment to be adopted, three-fourths of the states in the U.S would have to ratify it.
We rate the claim that the World Health Organization could “end the First Amendment” False.
This fact check was originally published by PolitiFact , which is part of the Poynter Institute. See the sources for this fact check here .

Opinion | Behind the scenes of CBS News’ interview with Pope Francis
The pope gave Norah O’Donnell a historic, hourlong interview from the Vatican. No topic was off-limits.

How a Supreme Court case most people likely have never heard of is reshaping LGBTQ+ rights
A 2020 Supreme Court case called Bostock v. Clayton County has led to a number of policy and legal shifts

CNN mourns the loss of commentator Alice Stewart
Stewart, a veteran political adviser who worked on several Republican presidential campaigns, was 58.

The best Pulitzer leads (or ledes) in 2024
Longtime writing coach Roy Peter Clark gives this year’s award to a gripping narrative about two octogenarians who died in a hurricane
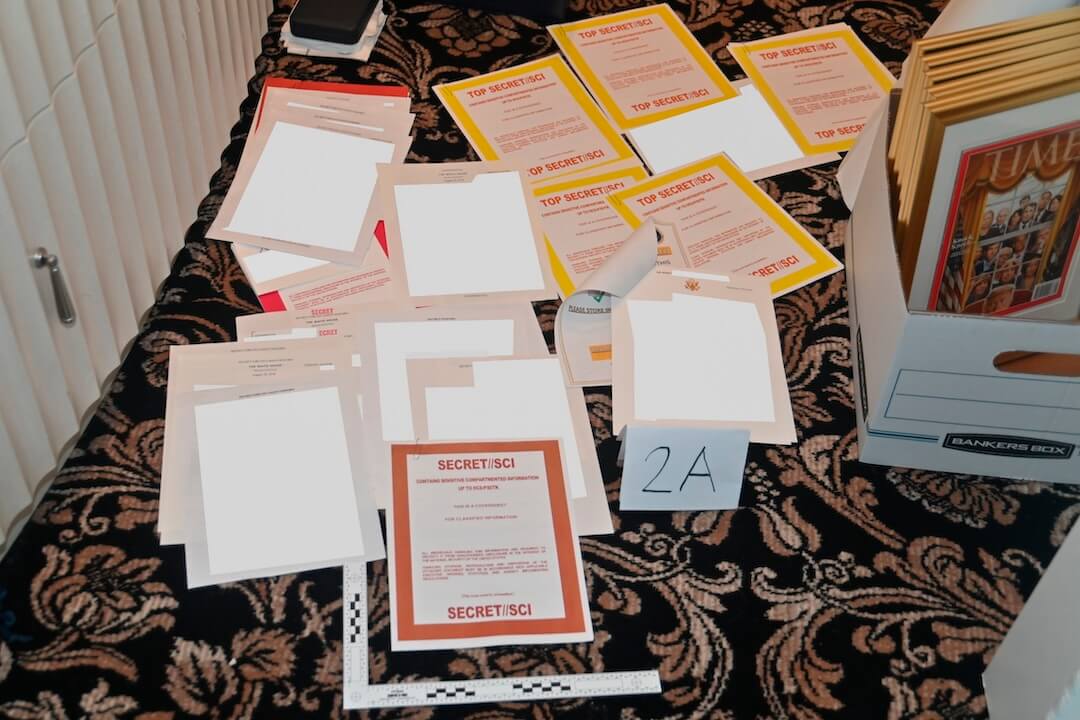
Benny Johnson’s claim that Joe Biden set up Donald Trump with classified documents is false
The conservative podcaster claimed the Biden administration framed former President Donald Trump by shipping boxes of classified documents to his home
You must be logged in to post a comment.
This site uses Akismet to reduce spam. Learn how your comment data is processed .
Start your day informed and inspired.
Get the Poynter newsletter that's right for you.
IMAGES
VIDEO
COMMENTS
The downloadable infographics below provide guidance on general and specific topics related to the pandemic. Stay aware of the latest COVID-19 information by regularly checking updates from WHO in addition to national and local public health authorities. Find out more about getting vaccinated: Advice for the public: COVID-19 vaccines
Reading time: 3 min (864 words) The COVID-19 pandemic has led to a dramatic loss of human life worldwide and presents an unprecedented challenge to public health, food systems and the world of work. The economic and social disruption caused by the pandemic is devastating: tens of millions of people are at risk of falling into extreme poverty ...
While the pandemic has underscored that vaccination is one of the most cost-effective public health interventions, we have already seen backsliding in routine immunization. In 2020, over 23 million children missed out on essential vaccines - an increase of nearly 4 million from 2019, with decades of progress tragically eroded.
Resilient health systems, built on robust primary health care, are a vital first line of defence against outbreaks with epidemic and pandemic potential; but they're also essential for promoting health, preventing communicable and noncommunicable diseases, and for reducing inequalities and inequities. In practice, this means a resilient health ...
Questions and answers about COVID-19 vaccine guidelines, development, and safety. Testing . NIH's role in developing accurate, widely available COVID-19 tests. ... The latest information on mental health during the COVID-19 pandemic. Search NIH COVID-19 Articles and Resources Scroll down the page to view all COVID-19 articles, stories, and ...
In times of crisis, communication by leaders is essential for mobilizing an effective public response. During the COVID-19 pandemic, compliance with public health guidelines has been critical for ...
Preventing the spread of COVID-19 requires persuading the vast majority of the public to significantly change their behavior in numerous, costly ways. Many efforts to encourage behavior change - public service announcements, social media posts, speeches, billboards - involve relatively short, persuasive messages. Here, we report results of five experimental tests (N = 5,351) of […]
Summary. Any communication in COVID-19 is crucial whether from government to people, from media to people, people to people, doctor to patient, within families and so on. Effective communication emphasizes the importance of content, accuracy, comprehensive signs, symbols, language, culture, and semiotic rules.
Speak the same language the public does. Communication is difficult when people are not speaking the same language. In the pandemic, we have seen this play out in two major ways. First: Scientists ...
We look forward to working with you to achieve that goal. Thank you. Regulated Product (s) Speech by Commissioner Stephen M. Hahn "The Critical Role of Health Care Professionals During the COVID ...
Push-ups, sit-ups, jumping-jacks and more exercises are great ways to stay fit away from the gym. Other ideas include: Walk briskly around the house or up and down the stairs for 10-15 minutes 2-3 times per day. Dance to your favorite music. Join a live exercise class on YouTube.
Three years ago this month, the virus that causes COVID-19 was first detected, the UN chief reminded on Tuesday, the International Day of Epidemic Preparedness. "The costs have been catastrophic", Secretary-General António Guterres said in a statement marking the day. Since the pandemic struck, he pointed out that millions of lives have ...
Coronavirus disease (COVID-19) is an infectious disease caused by the SARS-CoV-2 virus. Most people infected with the virus will experience mild to moderate respiratory illness and recover without requiring special treatment. However, some will become seriously ill and require medical attention. Older people and those with underlying medical ...
This investigation into the reception of public health messaging, which applies established health communications strategies in the context of COVID-19, enables us to make key recommendations for message writers, as we outline in 5.1. Further, our study has implications for applied CL, which we discuss in 5.2. 5.1.
Under this law, Section 31 stipulates that, where there is a pandemic or epidemic, the Minister of Health may make rules to regulate the response to contain the pandemic. By announcing these measures, I added a legal impetus to our ongoing efforts to prevent, contain and manage coronavirus which is wreaking havoc globally.
Short 2-Minute Speech on Covid 19 for Students. The coronavirus, also known as Covid - 19, causes a severe illness. Those who are exposed to it become sick in their lungs. A brand-new virus is having a devastating effect throughout the globe. It's being passed from person to person via social interaction.
In December 2019, the 2019 novel coronavirus disease (COVID-19) caused by novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) emerged in China, followed by a rapid spread all over the world. On March 11, 2020, the World Health Organization (WHO) raised its pandemic alert. As of April 11, 2020, COVID-19 had caused over 95,269 ...
The strength of the study lies in its large sample size, recruited during a crucial period—the early stage of the COVID-19 outbreak in Saudi Arabia. Nevertheless, this was an online self-reported survey conducted during lockdown due to pandemic, and this affected our outreach to the general population.
They also outline specific actions to prepare health systems, according to each of the "4 Cs" - no cases, sporadic cases, clusters of cases, and community transmission. These guidelines provide a wealth of practical information on screening and triage, referral, staff, supplies, standard of care, community engagement and more.
19. Summit. Briefing Room. Speeches and Remarks. Residence Library. (Prerecorded) THE PRESIDENT: Hello, everyone. Thank you for joining together for the second Global COVID-19 Summit. You know ...
The economic and social disruption caused by the COVID-19 pandemic is having major impacts on people's livelihoods and their health. As of 18 April 2021, there have been 140,322,903 confirmed ...
As you know, the first major speech I gave after my election as Director-General in 2017 was at the World Leaders Forum at Columbia, on the subject of health security. I began my remarks by describing the 1918 flu pandemic, which erupted during the First World War, and although it killed more people than the war itself, the pandemic was quickly ...
Such articles convey messages from governors, public health experts, physicians, COVID-19 patients, and residents of outbreak areas, encouraging people to stay at home. This is the first study to examine which narrator's message is most persuasive in encouraging people to do so during the COVID-19 pandemic and social lockdown.
A March 28 WHO press release said the pandemic agreement's draft will continue to be refined ahead of the World Health Assembly, set for May 27 to June 1 in Geneva, Switzerland. An April draft ...