Violence against women must stop; five stories of strength and survival

Facebook Twitter Print Email
Conflicts, humanitarian crises and increasing climate-related disasters have led to higher levels of violence against women and girls (VAWG), which has only intensified during the COVID-19 pandemic, bringing into sharp focus the urgent need to stem the scourge.
Globally, nearly one-in-three women have experienced violence, with crises driving the numbers even higher.
Gender-based violence (GBV), the most pervasive violation of human rights, is neither natural, nor inevitable, and must be prevented.
Marking the 16 Days of Activism to combat violence against women and girls, UN Women is showcasing the voices of five survivors, each of whose names has been changed to protect their identity. Be forewarned that each character sketch includes descriptions of gender-based violence.

‘Convinced’ she would be killed
From the Argentine province of Chaco, 48-year-old mother of seven, Diana suffered for 28 years before finally deciding to separate from her abusive partner.
“I wasn't afraid that he would beat me, I was convinced that he would kill me,” she said.
At first, she hesitated to file a police complaint for fear of how he might react, but as she learned more about the services provided by a local shelter, she realized that she could escape her tormentor. She also decided to press charges.
Living with an abusive father, her children also suffered psychological stress and economic hardship.
Leaving was not easy, but with the support of a social workers, a local shelter and a safe space to recover, Diana got a job as an administrative assistant in a municipal office.
Accelerate gender equality
- Violence against women and girls is preventable.
- Comprehensive strategies are needed to tackle root causes, transform harmful social norms, provide services for survivors and end impunity.
- Evidence shows that strong, autonomous women’s rights movements are critical to thwarting and eliminating VAWG.
- The Generation Equality Forum needs support to stem the VAWG violence.
“I admit that it was difficult, but with the [mental health] support, legal aid and skills training, I healed a lot,” she explained.
Essential services for survivors of domestic violence are a lifeline.
“I no longer feel like a prisoner, cornered, or betrayed. There are so many things one goes through as a victim, including the psychological [persecution] but now I know that I can accomplish whatever I set my mind to”.
Diana is among 199 women survivors housed at a shelter affiliated with the Inter-American Shelter Network, supported by UN Women through the Spotlight Initiative in Latin America. The shelter has also provided psychosocial support and legal assistance to more than 1,057 women since 2017.
Diana’s full story is here .
Survivor now ‘excited about what lies ahead’
Meanwhile, as the COVID-19 pandemic swept through Bangladesh, triggering a VAWG surge, many shelters and essential services shut down
Romela had been married to a cruel, torturous man.
“When I was pregnant, he punched me so hard I ended up losing my baby...I wanted to end my life”, she said.
She finally escaped when her brother took her to the Tarango women’s shelter, which in partnership with UN Women, was able to expand its integrated programme to provide safe temporary accommodations, legal and medical services, and vocational training to abused women who were looking for a fresh start.
Living in an abusive relationship often erodes women’s choices, self-esteem and potential. Romela had found a place where she could live safely with her 4-year-old daughter.
Opening a new chapter in her life, she reflected, “other people always told me how to dress, where to go, and how to live my life. Now, I know these choices rest in my hands”.
“ I feel confident, my life is more enjoyable ,” said the emancipated woman.
Tarango houses 30–35 survivors at any given time and delivers 24/7 services that help them recover from trauma, regain their dignity, learn new skills, and get job placement and a two-month cash grant to build their economic resilience.
“Our job is to make women feel safe and empowered, and to treat them with the utmost respect and empathy,” said Programme Coordinator Nazlee Nipa.
Click here for more on her story.

Uphill battle with in-laws
Goretti returned to western Kenya in 2001 to bury her husband and, as dictated by local culture, remained in the family’s homestead.
“But they wouldn’t give me food. Everything I came with from Nairobi – clothes, household items – was taken from me and divided between the family,” she recounted.
For nearly 20 years after her husband’s death, Goretti was trapped in a life of abuse until her in-laws they beat her so badly that she was hospitalized and unable to work.
Afraid to go to law enforcement, Goretti instead reached out to a local human rights defender, who helped her get medical attention and report the case to the local authorities.
They wouldn’t give me food. Everything...was taken from me and divided between the family – Survivor
However, she quickly discovered that her in-laws had already forged with the police an agreement in her name to withdraw the case.
“But I cannot even write”, Goretti said.
Human rights defenders in Kenya are often the first responders to violations, including GBV. Since 2019, UN Women and the UN Office of the High Commissioner for Human Rights ( OHCHR ) have been supporting grass-roots organizations that provide legal training and capacity-building to better assist survivors.
In addition to reporting the issue to local police and the courts, human rights defender Caren Omanga, who was trained by one of these organizations, also contacted the local elders.
“I was almost arrested when confronting the officer-in-charge”, Ms. Omanga explained. But knowing that the community would be against Goretti, she started “the alternative dispute-resolution process, while pushing the case to court”.
Finally, with her case settled out of court, Goretti received an agreement granting her the property and land title that she had lost in her marriage dowry, and the perpetrators were forced to pay fines to avoid prison.
“It is like beginning a new life after 20 years, and my son is feeling more secure… I’m thinking of planting some trees to safeguard the plot and building a poultry house”, she said.
Read Goretti’s story in its entirety here.
 speaks with Caren Omanga of the Nyando Social Justice Centre in Kenya.")
Raising consciousness
In Moldova, sexual harassment and violence are taboo topics and, fearing blame or stigmatization, victims rarely report incidents.
At age 14, Milena was raped by her boyfriend in Chisinau. She was unaware that her violation was a sexual assault and continued to see her abuser for another six months before breaking up. Then she tried to forget it.
“This memory was blocked, as if nothing happened”, until two years later, upon seeing an Instagram video that triggered flashbacks of her own assault, she said.
Almost one-in-five men in Moldova have sexually abused a girl or a woman, including in romantic relationships, according to 2019 research co-published by UN Women.
Determined to understand what had happened to her, Milena learned more about sexual harassment and abuse, and later began raising awareness in her community.
Last year, she joined a UN Women youth mentorship programme, where she was trained on gender equality and human rights and learned to identify abuse and challenge sexist comments and harassment.
Milena went on to develop a self-help guide for sexual violence survivors , which, informed by survivors aged 12 – 21, offers practical guidance to seek help, report abuse, and access trauma recovery resources.
Against the backdrop of cultural victim-blaming, which prevents those who need it from getting help, the mentoring programme focuses on feminist values and diversity, and addresses the root causes of the gender inequalities and stereotypes that perpetuate GBV and discrimination.
“The programme has shown that youth activism and engagement is key to eliminating gender inequalities in our societies”, explained Dominika Stojanoska, UN Women Country Representative in Moldova.
Read more about Milena here .
Support survivors, break the cycle of violence
A 2019 national survey revealed that only three-out-of-100 sexual violence survivors in Morocco report incidents to the police as they fear being shamed or blamed and lack trust in the justice system.

Layla began a relationship with the head of a company she worked for. He told her he loved her, and she trusted him.
“But he hit me whenever I disagreed with him. I endured everything, from sexual violence to emotional abuse…he made me believe that I stood no chance against him”, she said.
Pregnant, unmarried and lonely, Layla finally went to the police.
To her great relief, a female police officer met her, and said that there was a solution.
“I will never forget that. It has become my motto in life. Her words encouraged me to tell her the whole story. She listened to me with great care and attention”, continued Layla.
She was referred to a local shelter for single mothers where she got a second chance.
Two years ago, she gave birth to a daughter, and more recently completed her Bachelor’s Degree in mathematics.
“I was studying while taking care of my baby at the single mother’s shelter”, she said, holding her daughter’s hand.
UN Women maintains that building trust and confidence in the police is an integral part of crime prevention and community safety.
When professionally trained police handle GBV cases, survivors are more likely to report abuse and seek justice, health and psychosocial services that help break the cycle of violence while sending a clear message that it is a punishable crime.
Over the past few years, the General Directorate of National Security, supported by UN Women, has restructured the national police force to better support women survivors and prevent VAWG.
Today, all 440 district police stations have dedicated personnel who refer women survivors to the nearest specialized unit.
“It takes a lot of determination and courage for women to ask the police for support”, said Saliha Najeh, Police Chief at Casablanca Police Unit for Women Victims of Violence, who, after specialized training through the UN Women programme, now trains her police officers to use a survivor-centred approach in GBV cases.
As of 2021, 30 senior police officers and heads of units have been trained through the programme.
“Our role is to give survivors all the time they need to feel safe and comfortable, and for them to trust us enough to tell their story”, she said.
Prompted by the COVID-19 pandemic, Morocco has also expanded channels for survivors to report and access justice remotely through a 24-hour toll-free helpline, an electronic complaints mechanism, and online court sessions.
Click here for the full story.
These stories were originally published by UN Women.
- violence against women
- gender-based violence

SAFETY ALERT: If you are in danger, please use a safer computer and consider calling 911. The National Domestic Violence Hotline at 1-800-799-7233 / TTY 1-800-787-3224 or the StrongHearts Native Helpline at 1−844-762-8483 (call or text) are available to assist you.
Please review these safety tips .

Research & Evidence

NRCDV works to strengthen researcher/practitioner collaborations that advance the field’s knowledge of, access to, and input in research that informs policy and practice at all levels. We also identify and develop guidance and tools to help domestic violence programs and coalitions better evaluate their work, including by using participatory action research approaches that directly tap the diverse expertise of a community to frame and guide evaluation efforts.

Safety & Privacy in a Digital World

Immigrant Survivors of Domestic Violence

Teen Dating Violence

Housing and Domestic Violence

Domestic Violence in LGBTQ Communities

Trans and Non-Binary Survivors

The Difference Between Surviving & Not Surviving

Earned Income Tax Credit & Other Tax Credits

For an extensive list of research & evidence materials check out the research & statistics section on VAWnet
The Domestic Violence Evidence Project (DVEP) is a multi-faceted, multi-year and highly collaborative effort designed to assist state coalitions, local domestic violence programs, researchers, and other allied individuals and organizations better respond to the growing emphasis on identifying and integrating evidence-based practice into their work. DVEP brings together research, evaluation, practice and theory to inform critical thinking and enhance the field's knowledge to better serve survivors and their families.
The Community Based Participatory Research Toolkit (CBPR) is for researchers and practitioners across disciplines and social locations who are working in academic, policy, community, or practice-based settings. In particular, the toolkit provides support to emerging researchers as they consider whether and how to take a CBPR approach and what it might mean in the context of their professional roles and settings. Domestic violence advocates will also find useful information on the CBPR approach and how it can help answer important questions about your work.

For over two decades, the National Resource Center on Domestic Violence has operated VAWnet , an online library focused on violence against women and other forms of gender-based violence. VAWnet.org has long been identified as an unparalleled, comprehensive, go-to source of information and resources for anti-violence advocates, human service professionals, educators, faith leaders, and others interested in ending domestic and sexual violence.

Safe Housing Partnerships , the website of the Domestic Violence and Housing Technical Assistance Consortium , includes the latest research and evidence on the intersection of domestic and sexual violence, housing, and homelessness. You can also find new research exploring different aspects of efforts to expand housing options for domestic and sexual violence survivors, including the use of flexible funding approaches, DV Housing First and rapid rehousing, DV Transitional Housing, and mobile advocacy.
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
10 Working with Survivors of Gender-Based Violence
Dessie clark, ph.d., & joshua brown, lcsw, the purpose of this case study is to explore the process and outcomes of a collaboration between researchers and a community-based organization serving survivors of gender-based violence, fort bend women’s center., the big picture.

Gender-based violence is a rapidly growing social concern and even more so as the world continues to grapple with the effects of Covid-19. The implications of gender-based violence are too numerous to name here, but there are several special considerations for this population, including attrition (this population can be more transient than others), high caseload and rate of burnout for front line workers, as well as the physical and psychological effects of abuse, including traumatic brain injury (TBI) and initial reluctance to trust others. Further, gaps in existing work with survivors of gender-based violence include a mismatch between the expectations of researchers and the realities of those who are on the frontlines in these organizations and the people that they serve. The purpose of this case study is to explore the process and outcomes of a collaboration between researchers and a community-based organization serving survivors of gender-based violence, Fort Bend Women’s Center . We propose that focusing attention on communication, trust, buy-in, and burnout are critical for collaborations between researchers and community organizations that serve survivors of gender-based violence.
It is important to understand that collaborations, such as the one detailed in this case study, do not begin by happenstance. Strong collaborations can take time to develop. For this reason, the authors find it important to explain the origins of this project. In 2012, Abeer Monem (now former) Chief Programs Officer of the Fort Bend Women’s Center (FBWC) began to explore reasons why a portion of the agency’s Intimate Partner Violence (IPV) survivors were struggling to progress toward self-sufficiency, despite the agency’s existing program offerings such as case management and counseling. As the agency explored the reasons behind the lack of progress, it became clear that one of the main reasons could be potential traumatic brain injury (TBI) in the survivor population. Eager to confirm their suspicion, agency personnel embarked on the discovery and research phases of the intervention’s lifecycle.
It was first deemed necessary to determine if agency survivors indeed exhibited a likelihood of traumatic brain injury. FBWC personnel began administering the HELPS Screening Tool for Traumatic Brain Injury (HELPS) (M. Picard, D. Scarisbrick, R. Paluck, International Center for the Disabled, TBI-NET, and U.S. Department of Education, Rehabilitation Services Administration). The HELPS Screening Tool is a simple tool designed to be given by professionals who are not TBI experts. FBWC personnel began by offering the HELPS upon intake to survivors seeking services. The initial findings found that over 50% of survivors screened positive for a potential brain injury incident. With this knowledge, FBWC program leadership began exploring neurofeedback as an innovative approach to assisting survivors exhibiting symptoms of TBI. FBWC approached another non-profit organization that was focused on researching and propagating neurofeedback in public school-based settings. After deliberations between leadership groups, a budget and project plan was finalized.
FBWC leadership began seeking funding from various sources and, after several attempts over approximately 18 months, two sources (one governmental, one non-governmental) agreed to fund the initial work of the neurofeedback project. Initial funding covered the neurofeedback equipment as well as the cost of setup, training, and mentoring by a board-certified neurofeedback clinician. In late 2014, FBWC began an initial pilot program to determine the impact and efficacy of a neurofeedback training program for Intimate Partner Violence (IPV) survivors with potential brain injury in an agency setting.
In 2017, I (Dessie Clark) traveled to Houston, Texas where she was introduced to Abeer Monem, the previous Chief Programs Officer of FBWC. During this meeting, Abeer shared information about an innovative neurofeedback program that was happening at FBWC. She described the approach and noted that they had been collecting data on the program to try to assess efficacy and impact. Dessie was intrigued and agreed to visit the site later that week. Upon arrival, Dessie was introduced to Joshua Brown, a board-certified neurofeedback clinician, who was the Director of Special Initiatives (now Chief Programs Officer) and one of the founders of the neurofeedback program. After multiple discussions, an agreement was reached between the two parties to begin a collaboration.

Community Assets & Needs
Fort Bend Women’s Center provides comprehensive services for survivors such as emergency shelter, case management, counseling, housing services, and legal aid. It is important to acknowledge that there are components of Fort Bend Women’s Center that are unique to the way the agency approaches service provision. Community assets will vary widely, even amongst similar populations. That being said, we believe the following assets are important to intimate partner violence survivors generally. First, FBWC emphasizes a trauma-informed care approach to working with survivors. The service model is voluntary (as opposed to other models that may have mandatory or compulsory services) and non-judgmental. Specifically, at FBWC, there was existing trust between staff and survivors. This is largely due to a rules reduction , trauma-informed care model that focuses on enhancing internal motivation in survivors and open and honest communication with staff. This helps to create a culture where survivors feel willing and able to be more open about their experiences and the challenges they are facing. Important elements of this model include the offering of voluntary services and non-judgmental advocacy. This model has led to survivors developing a vested interest in the success of FBWC as an agency. Many survivors participated in the research because they felt motivated to share with others their positive experiences at FBWC. Also, many survivors return to FBWC to volunteer following service provision. Please note that the intrinsic motivation to stay involved with FBWC is not a common phenomenon in this community. This illustrates the importance of continual work on trust, safety, and confidentiality.
The IPV survivor community has myriad needs, and no one IPV community will have the same needs. For this partnership, there were several key needs of the survivors at Fort Bend Women’s Center that became vital to address in order to successfully implement the partnership. These needs included trust, safety, confidentiality, and adaptability. Given the trauma that survivors have experienced, these components need to be taken into consideration in interactions with other survivors, staff, and members of the research team.
The survivor population at Fort Bend Women’s Center have experienced violence from a family member and/or sexual assault. FBWC data suggests that over half of the survivors seeking services at FBWC have experienced multiple traumatic experiences. Additionally, some survivors may have had difficult experiences with the justice system, the medical establishment, and other helping professionals. Experiences of trauma can cause distrust from the survivor when seeking services. Additionally, there is a high incidence of mental health disorders in survivors, including paranoia, that can impede the creation of a trusting relationship. Establishing trust became a vital step in survivor recruitment. For effective recruitment, it was imperative that survivors trusted that their information would be kept in confidence and that what they were being asked to participate in would not harm them. As previously mentioned, a culture of trust already existed between survivors and staff. The research team was able to build on this by including staff in the research collaboration. Staff members were included in project development, which allowed them to have a deeper understanding of the work. Staff’s enthusiasm for the collaboration, which was shared with survivors, helped extend the pre-existing trust that survivors had with staff members to the research collaboration.
Safety is of utmost importance to survivors who are fleeing violence. While one might only think of physical safety with this population, it is also important to take psychological safety into account. Steps were taken in this program to ensure that participating survivors understood the likelihood of any psychological harm due to sharing their traumatic experiences. Mental health staff was identified on a rotating basis to act as an on-call resource should survivors need it.
Confidentiality
Confidentiality of personal information directly involves trust and safety. Many survivors in our program feared for their lives and did not want anyone to know where they were or what they were doing. It is important when working with this population to ensure confidentiality. This is not only ethically and legally important, it is also important in building a long-lasting program. When thinking about effective confidentiality, one should consider their applicable agency, state, and federal confidentiality rules and regulations. At a minimum, it is important to execute a confidentiality agreement with the participant.
Collaborative Partners
To begin the process of engaging in effective research collaborations, it is often difficult to identify an effective community partner, and it is a somewhat arduous process. While individuals and organizations in academia understand the merits of research, this is not always the case for community organizations. Even in cases where community organizations recognize these benefits, there may be barriers, such as trust, due to historical harms done to communities by researchers. Additionally, community organizations often face strains due to limited resources or capacity to support research which researchers may fail to acknowledge or understand. These issues can create barriers for researchers who are interested in partnering with organizations that have survivor populations. This also causes issues for community organizations who may be less likely to have access to research, including best practices, given academic publishing practices.
Building understanding and trust between researchers and community partners is at the heart of a successful collaboration. A solid research partnership with a community organization requires buy-in from both sides. Whether from the perspective of the community organization or the researcher, it is imperative to find a partner that communicates effectively. This involves clearly defining each party’s expectations upfront, making sure that the terms that are used are clearly understood (including any potential jargon), and discussing the importance of flexibility in timelines. A great example of the lack of work on building understanding and trust is the story of the (now-defunct) nonprofit Southwest Health Technology Foundation (SWHTF) in which one author, Joshua Brown, was an employee. SWHTF was a small organization that was focused on evaluating the effectiveness of neurofeedback in existing systems (such as public schools). SWHTF began several data-driven pilot projects without the assistance of a research partner. These data showed the potential positive effects of neurofeedback interventions on behavior and academic performance. However, these data never saw the light of day. SWHTF leadership attempted to partner with four different research institutions to analyze the data. All four attempts ultimately failed without yielding tangible results. This was due to a failure on the part of SWHTF and the researchers to build trust and understanding through defining clear expectations, clearly understanding each party’s role, and agreeing on expected outcomes.
An important part of building trust is approaching a partnership with strategies that are aimed at the education of staff and survivors who will be involved. While SWHTF is a relevant example, the focus of this case study is the project conducted with Fort Bend Women’s Center (FBWC). We found the most effective approach to building trust and understanding was to focus on educating staff about our project first. We identified the case managers as those staff who have the most contact with survivors and have built up the most trust. When educating staff members, we found that it wasn’t as important that they fully understood all the specifics of the project but, rather, that they had enough of a basic level of knowledge about the project to introduce the information to the survivor. Because case managers had built up trust with the survivors, the survivors were much more likely to take the recommendation of the case manager and enroll in the program. Because our case managers were not subject experts, survivors were willing to speak to researchers even without an understanding of the specifics. The specifics were provided by researchers and program staff before enrollment.
In order to understand how a community navigates issues related to gender-based violence, it is important to understand the ways in which the culture of that community may impact their perspective. The key stakeholders in this project included the funding entities, the Chief Programs Officer, the Neurofeedback program Lead, and members of the Neurofeedback team. The population consisted of survivors of gender-based violence; both those who had completed a neurofeedback program and those who had not yet done so but desired to do so in the future. This research collaboration was between researchers at Michigan State University and Fort Bend Women’s Center. The organization, which served as the primary setting for the project, provides emergency shelter, housing/rental assistance, and supportive services. The project was predominantly made up of those located within the agency as staff members while researchers at Michigan State University primarily served as guides and consultants for the research portion of the project. For this project, funders included the Texas Health and Human Services Commission, the George Foundation, the Simmons Foundation, and the Office for Victims of Crime.
Project Description
This case study involved a multi-year collaboration. During the initial six-months, a series of site visits were conducted with the goal of researchers getting to know staff members of the community organization, as well as the survivors who received services from the organization. Before engaging in any research, a multi-day feedback session was held in which staff members from the organization gave feedback on the research including the approach, questions, assessment tools, and logistics of how the research would be conducted. In these sessions, it became clear that given the population being served at this site, to include high numbers of disabled or immigrant survivors, there would need to be adjustments for accessibility and safety. Other barriers specific to this collaboration included staff burdens, the distance between researcher and community partner, and various considerations given the population such as trauma responses, trauma history, and the relatively transient nature of the population. Additionally, the research and data collection experience of the staff at the community organization was limited. These conversations were critical in helping the community organization familiarize themselves with the research and the researcher obtain a better understanding of the unique strains the organization was facing in conducting the research. As such, novel processes had to be developed and reinforced to ensure adequate data collection and analysis. We involved considerations for a variety of perspectives that may be shared by survivors in our data collection approach. We would do this in the future, with more frequent check-ins with participants and staff.
The collaboration consisted of frequent communication between the researchers and the organization. Additionally, site visits happened semi-annually. Key outcomes included – efficacy of the intervention was established, adaptive technology was created, and we found evidence of a successful collaboration. The neurofeedback intervention resulted in statistically significant decreases in depression, anxiety, PTSD, and disability symptomology for survivors. Survivors also experienced normalization of brain activity. This provides evidence that neurofeedback can benefit the well-being of survivors. Given the distance between Michigan and Texas, a system was created for checking in, transferring data, and ensuring that all necessary tasks were completed. A particularly novel component of this collaboration was the creation of an app for mobile phones that allowed for data to be transferred securely from Texas, in areas where Wi-Fi may not be present, to Michigan. The creation of a mobile phone app can be replicated. This was an important aspect of conducting research with a population where safety was critical, and Wi-Fi may not always be accessible. Finishing the project, and creating tools to do so, is in itself an indicator that the collaboration was successful. However, this project resulted in a host of other products such as publications, technical reports, presentations, and an awarded grant which also indicate that this collaboration produced well-recognized resources. Not a traditional metric, but one of great importance to the authors is the fact that both the agency and the researchers wish to work together in the future.
Lessons Learned
Over the course of the 3-year collaboration, we learned many lessons about conducting rigorous research with community partners who serve survivors of gender-based violence. However, we highlight the four biggest takeaways from our collaboration – (1) communication, (2) trust, (3) buy-in, and (4) resources. It’s important to note that there is no such thing as a perfect collaboration. Collaborations can be successful, produce important results, and still face challenges. It’s important to note that there is no such thing as a perfect collaboration. Collaborations can be successful, produce important results, and still face challenges. That is true of our collaboration, in which we did face challenges. For domestic violence agencies, there is one overarching consideration that impacts the four takeaways we will discuss below – turnover and movement of staff. Turnover and movement of staff is relatively common in community agencies and that means that there is a constant need to set and reset expectations to make sure everyone has the same information about the project and what is expected of them. These expectations need to be reinforced frequently to ensure there are no issues that need to be addressed. For example, in the first 3 years of our collaboration, we experienced 3 different neurofeedback team leads and have seen the neurofeedback clinical team have full turnover twice. Our experience underlines the importance of consistently resetting expectations.
Communication
We have found in collaborations with multiple parties, particularly those that are conducted long-distance, communication is perhaps the most important ingredient for success. How do you work collaboratively when not in the same space? For us, it was critical to use technology. We used secure platforms to share information and have important conversations. However, having conversations is not enough. It is important these conversations do not use jargon. For example, there are certain technical terms that researchers or practitioners may use which are not clear and can lead to confusion. It’s also important to share perspectives on what the priorities are for different parties. For example, researchers may be worried about things such as missing data whereas counselors may be more willing to collect minimal data in an effort to move on to the next survivor more quickly or to protect survivor confidentiality. Communication is complicated, especially at a distance. It’s important to realize you may do the best you can and still have problems communicating. Defining modes of communication, and what expectations are, is also critical. For example, what constitutes an email versus a call, how frequent those communications will be, and what expectations are for when those communications will be returned.
It is critical that there is trust between all parties. The survivors must trust the community partner and the researchers, the community partners must trust the researchers, and the researchers must trust the community partners and the survivors. This can create a complex web of dynamics that can be vulnerable to changes and miscommunications. In our collaboration, there were moments where trust and understanding between the researchers and the community partners were limited. In retrospect, it was important for community partners and researchers to sit down and share their perspectives and approach to work. For example, researchers may be more focused on details like completing paperwork properly or recruitment and retention of participants. Whereas, community partners may be more focused on completing interventions or connecting survivors to resources. In both cases, these duties are appropriate for the position but given the rapidly changing needs of survivors, the priorities may not be in alignment across groups. It is critical for both parties to understand where the other is coming from and trust that the necessary steps for the project will be completed. Collaborations should tackle this issue by communicating freely and openly and not resulting in micromanaging or avoiding these issues. Collaborators must trust that all members of the collaboration will do their part and be transparent if and when issues arise. In our case, this impacted survivors’ access to the project because at times, due to other survivor or agency demands, staff members were not actively talking to survivors about the project and what it may entail to become involved and learn more.
Ensuring that researchers, community stakeholders, and survivors have bought into the project and understand the project plan is important in ensuring things run smoothly. While the project itself may involve conducting research, it’s important to elicit feedback from the other collaborators at all aspects of the process. In our case, we asked staff members and survivors to provide feedback on the project design and survey. We hosted a multi-day training to talk through the process, the questions we were asking, and gather feedback on what we should know to inform the project moving forward. However, as referenced above, these agencies may experience frequent turnover of staff movement. As such, is it important to check in about buy-in over the course of the project – but particularly when there are transitions.
Working with community partners, who are often over-burdened and under-resourced, requires acknowledgment and supplementation from other collaborators. In our case, it was important for the researchers to design and adjust the project to best meet the needs of the community partner and survivors. We did this by:
- Taking over aspects of the project like data collection to the extent that was allowable given distance and travel,
- Hiring staff members as research assistants to help with data collection; and
- Creating a phone application that allowed for information necessary for the project to be directly transmitted to a secure server at MSU.
While for many of our lessons learned, we have concrete suggestions for future work, we do find ourselves with one lesson we have learned but have not solved. A constant challenge on this project was learning how to deal with staff burnout – both in their roles and in regard to the research project. For example, as we’ve mentioned staff at these agencies are often overburdened and under-resourced. Participating in research can exacerbate these issues and lead to a faster rate of burnout or what we observed and have called “research fatigue”. We believe that having a place to vent frustrations about the research project so they may be dealt with is a promising thought. However, this is a bit complicated as it seems that staff may be unsure of the appropriate avenue to share these concerns – whether it should be their agency supervisor or a member of the research team.
Research Process
A relatively unique aspect of this project was the willingness of staff to engage in all aspects of the research process. Members of FBWC were engaged throughout the entire process from project conceptualization to dissemination of information. The key stakeholder, Joshua Brown, was eager to be involved in research. However, this was only possible because Dessie Clark suggested the possibility and Joshua didn’t know that it is unusual for community partners to be involved. This highlights the importance for researchers and community partners to be talking about research, the degree to which each member wants to be involved, and what expectations will be. The authors of this chapter had many conversations about authorship on all the produced works and what workload and timeline would look like to live up to these expectations.
Looking Forward
As we continue to move forward, we would be remiss if we did not acknowledge the impacts of COVID-19 on the intimate partner survivors, the agencies (such as Fort Bend Women’s Center) that serve them, and research for those housed in a University setting. Before COVID-19 we imagined continuing our work in many of the same ways. We had applied for future grants and dreamed of expanding our work to examine the children’s neurofeedback program at Fort Bend Women’s Center. While we hope that eventually conducting our work, in-person, will continue, it seems prudent to reimagine what working together will look like in our altered state. It is the intention of the authors to continue collaborating. However, this may require adjusting to continue working in a virtual matter. Given the fact that technology has already been an important part of our process as long-distance partners, we hope that future work uses those technologies (digital survey platform, phone app for information transfer, etc.) to continue to collect important information that ultimately benefits survivors and their communities.
Recommendations
While gender-based violence is often examined at the individual level, communities play an important role in how gender-based violence is addressed and how survivors are supported. Communities can be a tremendous source of support for survivors by providing social support through which these individuals can access resources, and connect to services. In this way, communities have the potential to be a tremendous source of support for survivors. Or, in contrast, communities can impose substantial barriers on survivors and their families. Since structurally, communities are located closest to survivors, understanding how gender-based violence is addressed by, and within, communities is important in understanding and confronting gender-based violence as a society. The nature of this work was relatively clinical in nature (e.g. neurofeedback) where community relationships and community-engaged research are not a typical fixture. This effort provides suggestions for how those in clinical disciplines, like clinical psychology or social work, may conduct work with community psychologists that are more interdisciplinary in nature.
Further recommendations include:
- Examining how those who do more clinical/individual work may engage with communities,
- The use of technology to conduct and engage in community work, and
- How researchers may do work in communities that is rigorous, such as the waitlist control trial done here, and is not limited to that which can be done inside a lab.
A frequent conversation between the authors of this article was about the wall that exists between researchers and communities. Often, it is assumed that communities do not value or understand research. Or, conversely, that any research that can be done in community settings is not rigorous or worthwhile. Our experiences show the inaccuracy of these assumptions. Fort Bend Women’s Center created the neurofeedback program with research in mind. They implemented best practices and collected necessary data. While they didn’t have the resources to compile and analyze the data in ways that could be presented to the scientific community – they were certainly open and eager for the opportunity. Additionally, the research that has been done in this collaboration so far has been recognized widely and invited to contribute to special issues and conference keynotes – a marker of success in the scientific community. This was successful because people, located in very different spaces, were willing to discuss how they could meet in the middle to accomplish a common goal. The experiences of survivors happen in real-world settings and it was important to capture their lived experiences in that setting.
It is important to take the time on the front end to develop a plan. But, also, recognizing that plan likely will change. There should be explicit plans for action with turnover and communication. The priorities of the work should be established and reinforced. This includes defining what priorities are overlapping, and what priorities are important to researchers and community partners so they can work together effectively. Given the fluid nature of research, domestic violence organizations, and survivors it is important for everyone to be willing to adapt. Researchers may be forced to make changes to the research plan, particularly to meet staff and survivors’ needs. The agency may need to adapt to ensure that the research components fit into their own expectations and be willing to give feedback if they do not so adjustments can be made.
Implications for Community Psychology
There has been a multitude of promising results from this project including, establishing the efficacy of the intervention, creation of adaptive technology, and evidence of successful collaboration. In our case, researchers and community partners have published and presented in academic spaces and created a technical report for practitioners. Community psychology theory often focuses on engaging local communities that are relatively close to the research team. This case study has implications for how to do community-engaged research over a long distance using various technologies. This has the potential to further the conversation on how we can engage and work with communities when physical access may not be possible. This is important as funding and travel can pose barriers to certain populations and novel ways of doing this work may present additional opportunities for other researchers.
The authors of this case story believe that finding creative ways to manage mostly virtual relationships, as we have done here, has always been a critical component of doing community psychology work. However, as we wrote this chapter during COVID-19 we realized that what has been important to those of us striving to reach vulnerable populations in hard-to-reach locations is now a standard challenge. While community psychology has always pushed innovative ways to do community work, limited conversations have evolved on how adaptive technology could and should be used to try to ensure successful collaborations, particularly collaborations across distance.
From Theory to Practice Reflections and Questions
- Gender-based violence is a rapidly growing social concern and even more so as the world continues to grapple with the effects of Covid-19 (Clark & Brown, 2021). How does the discussion in this case study challenge your thinking regarding traumatic brain injury (TBI) and gender-based violence?
- Reflect upon conversations you have heard and/or had on gender-based violence. List 3-5 statements you have heard. Based on these statements what would you consider about society’s response to this issue? If you have not heard any stereotypical or other statements, research 3-5 statements and answer the same question.
- How would you go about creating an alternate setting to address this challenge in the community?
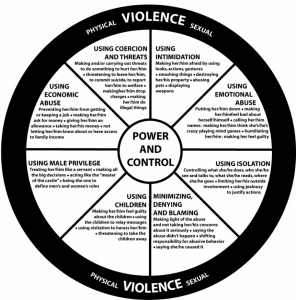
Domestic Abuse Intervention Project (n.d.).The Domestic Violence Power and Control Wheel https://www.thehotline.org/identify-abuse/power-and-control/
Case Studies in Community Psychology Practice: A Global Lens Copyright © 2021 by See Contributors Page for list of authors (Edited by Geraldine Palmer, Todd Rogers, Judah Viola, and Maronica Engel) is licensed under a Creative Commons Attribution 4.0 International License , except where otherwise noted.
Share This Book
Feedback/errata.
Comments are closed.
Important Safety Information
QUICK CLOSE at the top of the page will exit this site immediately and take you to google.co.uk.

This will not hide the fact that you have been on our website.
If you are worried someone will know you are trying to find help, please read our instructions on how to browse safely. Follow the "Browse safely" link at the top of the screen.
Continue to site
- Skip to navigation
- Skip to content
- Browse safely
In their own words
Sometimes it helps to read other people’s stories. These case studies of domestic abuse highlight some real stories.
Psychological abuse - Marianna's story
Physical abuse - jenny's story, sexual abuse - husna's story, financial abuse - halima's story, emotional abuse - jane's story.
Are you in an abusive relationship?
Women’s Aid have a checklist that can help you identify if you are in an abusive relationship.
- Are you in danger now?
- Are you looking for legal advice about domestic abuse?
- Are you looking for local support about domestic abuse?
- What is domestic abuse?
- Open access
- Published: 20 June 2023
A qualitative quantitative mixed methods study of domestic violence against women
- Mina Shayestefar 1 ,
- Mohadese Saffari 1 ,
- Razieh Gholamhosseinzadeh 2 ,
- Monir Nobahar 3 , 4 ,
- Majid Mirmohammadkhani 4 ,
- Seyed Hossein Shahcheragh 5 &
- Zahra Khosravi 6
BMC Women's Health volume 23 , Article number: 322 ( 2023 ) Cite this article
8359 Accesses
1 Altmetric
Metrics details
Violence against women is one of the most widespread, persistent and detrimental violations of human rights in today’s world, which has not been reported in most cases due to impunity, silence, stigma and shame, even in the age of social communication. Domestic violence against women harms individuals, families, and society. The objective of this study was to investigate the prevalence and experiences of domestic violence against women in Semnan.
This study was conducted as mixed research (cross-sectional descriptive and phenomenological qualitative methods) to investigate domestic violence against women, and some related factors (quantitative) and experiences of such violence (qualitative) simultaneously in Semnan. In quantitative study, cluster sampling was conducted based on the areas covered by health centers from married women living in Semnan since March 2021 to March 2022 using Domestic Violence Questionnaire. Then, the obtained data were analyzed by descriptive and inferential statistics. In qualitative study by phenomenological approach and purposive sampling until data saturation, 9 women were selected who had referred to the counseling units of Semnan health centers due to domestic violence, since March 2021 to March 2022 and in-depth and semi-structured interviews were conducted. The conducted interviews were analyzed using Colaizzi’s 7-step method.
In qualitative study, seven themes were found including “Facilitators”, “Role failure”, “Repressors”, “Efforts to preserve the family”, “Inappropriate solving of family conflicts”, “Consequences”, and “Inefficient supportive systems”. In quantitative study, the variables of age, age difference and number of years of marriage had a positive and significant relationship, and the variable of the number of children had a negative and significant relationship with the total score and all fields of the questionnaire (p < 0.05). Also, increasing the level of female education and income both independently showed a significant relationship with increasing the score of violence.
Conclusions
Some of the variables of violence against women are known and the need for prevention and plans to take action before their occurrence is well felt. Also, supportive mechanisms with objective and taboo-breaking results should be implemented to minimize harm to women, and their children and families seriously.
Peer Review reports
Violence against women by husbands (physical, sexual and psychological violence) is one of the basic problems of public health and violation of women’s human rights. It is estimated that 35% of women and almost one out of every three women aged 15–49 experience physical or sexual violence by their spouse or non-spouse sexual violence in their lifetime [ 1 ]. This is a nationwide public health issue, and nearly every healthcare worker will encounter a patient who has suffered from some type of domestic or family violence. Unfortunately, different forms of family violence are often interconnected. The “cycle of abuse” frequently persists from children who witness it to their adult relationships, and ultimately to the care of the elderly [ 2 ]. This violence includes a range of physical, sexual and psychological actions, control, threats, aggression, abuse, and rape [ 3 ].
Violence against women is one of the most widespread, persistent, and detrimental violations of human rights in today’s world, which has not been reported in most cases due to impunity, silence, stigma and shame, even in the age of social communication [ 3 ]. In the United States of America, more than one in three women (35.6%) experience rape, physical violence, and intimate partner violence (IPV) during their lifetime. Compared to men, women are nearly twice as likely (13.8% vs. 24.3%) to experience severe physical violence such as choking, burns, and threats with knives or guns [ 4 ]. The higher prevalence of violence against women can be due to the situational deprivation of women in patriarchal societies [ 5 ]. The prevalence of domestic violence in Iran reported 22.9%. The maximum of prevalence estimated in Tehran and Zahedan, respectively [ 6 ]. Currently, Iran has high levels of violence against women, and the provinces with the highest rates of unemployment and poverty also have the highest levels of violence against women [ 7 ].
Domestic violence against women harms individuals, families, and society [ 8 ]. Violence against women leads to physical, sexual, psychological harm or suffering, including threats, coercion and arbitrary deprivation of their freedom in public and private life. Also, such violence is associated with harmful effects on women’s sexual reproductive health, including sexually transmitted infection such as Human Immunodeficiency Virus (HIV), abortion, unsafe childbirth, and risky sexual behaviors [ 9 ]. There are high levels of psychological, sexual and physical domestic abuse among pregnant women [ 10 ]. Also, women with postpartum depression are significantly more likely to experience domestic violence during pregnancy [ 11 ].
Prompt attention to women’s health and rights at all levels is necessary, which reduces this problem and its risk factors [ 12 ]. Because women prefer to remain silent about domestic violence and there is a need to introduce immediate prevention programs to end domestic violence [ 13 ]. violence against women, which is an important public health problem, and concerns about human rights require careful study and the application of appropriate policies [ 14 ]. Also, the efforts to change the circumstances in which women face domestic violence remain significantly insufficient [ 15 ]. Given that few clear studies on violence against women and at the same time interviews with these people regarding their life experiences are available, the authors attempted to planning this research aims to investigate the prevalence and experiences of domestic violence against women in Semnan with the research question of “What is the prevalence of domestic violence against women in Semnan, and what are their experiences of such violence?”, so that their results can be used in part of the future planning in the health system of the society.
This study is a combination of cross-sectional and phenomenology studies in order to investigate the amount of domestic violence against women and some related factors (quantitative) and their experience of this violence (qualitative) simultaneously in the Semnan city. This study has been approved by the ethics committee of Semnan University of Medical Sciences with ethic code of IR.SEMUMS.REC.1397.182. The researcher introduced herself to the research participants, explained the purpose of the study, and then obtained informed written consent. It was assured to the research units that the collected information will be anonymous and kept confidential. The participants were informed that participation in the study was entirely voluntary, so they can withdraw from the study at any time with confidence. The participants were notified that more than one interview session may be necessary. To increase the trustworthiness of the study, Guba and Lincoln’s criteria for rigor, including credibility, transferability, dependability, and confirmability [ 16 ], were applied throughout the research process. The COREQ checklist was used to assess the present study quality. The researchers used observational notes for reflexivity and it preserved in all phases of this qualitative research process.
Qualitative method
Based on the phenomenological approach and with the purposeful sampling method, nine women who had referred to the counseling units of healthcare centers in Semnan city due to domestic violence in February 2021 to March 2022 were participated in the present study. The inclusion criteria for the study included marriage, a history of visiting a health center consultant due to domestic violence, and consent to participate in the study and unwillingness to participate in the study was the exclusion criteria. Each participant invited to the study by a telephone conversation about study aims and researcher information. The interviews place selected through agreement of the participant and the researcher and a place with the least environmental disturbance. Before starting each interview, the informed consent and all of the ethical considerations, including the purpose of the research, voluntary participation, confidentiality of the information were completely explained and they were asked to sign the written consent form. The participants were interviewed by depth, semi-structured and face-to-face interviews based on the main research question. Interviews were conducted by a female health services researcher with a background in nursing (M.Sh.). Data collection was continued until the data saturation and no new data appeared. Only the participants and the researcher were present during the interviews. All interviews were recorded by a MP3 Player by permission of the participants before starting. Interviews were not repeated. No additional field notes were taken during or after the interview.
The age range of the participants was from 38 to 55 years and their average age was 40 years. The sociodemographic characteristics of the participants are summarized in table below (Table 1 ).
Five interviews in the courtyards of healthcare centers, 2 interviews in the park, and 2 interviews at the participants’ homes were conducted. The duration of the interviews varied from 45 min to one hour. The main research question was “What is your experience about domestic violence?“. According to the research progress some other questions were asked in line with the main question of the research.
The conducted interviews were analyzed by using the 7 steps Colizzi’s method [ 17 ]. In order to empathize with the participants, each interview was read several times and transcribed. Then two researchers (M.Sh. and M.N.) extracted the phrases that were directly related to the phenomenon of domestic violence against women independently and distinguished from other sentences by underlining them. Then these codes were organized into thematic clusters and the formulated concepts were sorted into specific thematic categories.
In the final stage, in order to make the data reliable, the researcher again referred to 2 participants and checked their agreement with their perceptions of the content. Also, possible important contents were discussed and clarified, and in this way, agreement and approval of the samples was obtained.
Quantitative method
The cross-sectional study was implemented from February 2021 to March 2022 with cluster sampling of married women in areas of 3 healthcare centers in Semnan city. Those participants who were married and agreed with the written and verbal informed consent about the ethical considerations were included to the study. The questionnaire was completed by the participants in paper and online form.
The instrument was the standard questionnaire of domestic violence against women by Mohseni Tabrizi et al. [ 18 ]. In the questionnaire, questions 1–10, 11–36, 37–65 and 66–71 related to sociodemographic information, types of spousal abuse (psychological, economical, physical and sexual violence), patriarchal beliefs and traditions and family upbringing and learning violence, respectively. In total, this questionnaire has 71 items.
The scoring of the questionnaire has two parts and the answers to them are based on the Likert scale. Questions 11–36 and 66–71 are answered with always [ 4 ] to never (0) and questions 37–65 with completely agree [ 4 ] to completely disagree (0). The minimum and maximum score is 0 and 300, respectively. The total score of 0–60, 61–120 and higher than 121 demonstrates low, moderate and severe domestic violence against women, respectively [ 18 ].
In the study by Tabrizi et al., to evaluate the validity and reliability of this questionnaire, researchers tried to measure the face validity of the scale by the previous research. Those items and questions which their accuracies were confirmed by social science professors and experts used in the research, finally. The total Cronbach’s alpha coefficient was 0.183, which confirmed that the reliability of the questions and items of the questionnaire is sufficient [ 18 ].
Descriptive data were reported using mean, standard deviation, frequency and percentage. Then, to measure the relationship between the variables, χ2 and Pearson tests also variance and regression analysis were performed. All analysis were performed by using SPSS version 26 and the significance level was considered as p < 0.05.
Qualitative results
According to the third step of Colaizzi’s 7-step method, the researcher attempted to conceptualize and formulate the extracted meanings. In this step, the primary codes were extracted from the important sentences related to the phenomenon of violence against women, which were marked by underlining, which are shown below as examples of this stage and coding.
The primary code of indifference to the father’s role was extracted from the following sentences. This is indifference in the role of the father in front of the children.
“Some time ago, I told him that our daughter is single-sided deaf. She has a doctor’s appointment; I have to take her to the doctor. He said that I don’t have money to give you. He doesn’t force himself to make money anyway” (p 2, 33 yrs).
“He didn’t value his own children. He didn’t think about his older children” (p 4, 54 yrs).
The primary code extracted here included lack of commitment in the role of head of the household. This is irresponsibility towards the family and meeting their needs.
“My husband was fired from work after 10 years due to disorder and laziness. Since then, he has not found a suitable job. Every time he went to work, he was fired after a month because of laziness” (p 7, 55 yrs).
“In the evening, he used to get dressed and go out, and he didn’t come back until late. Some nights, I was so afraid of being alone that I put a knife under my pillow when I slept” (p 2, 33 yrs).
A total of 246 primary codes were extracted from the interviews in the third step. In the fourth step, the researchers put the formulated concepts (primary codes) into 85 specific sub-categories.
Twenty-three categories were extracted from 85 sub-categories. In the sixth step, the concepts of the fifth step were integrated and formed seven themes (Table 2 ).
These themes included “Facilitators”, “Role failure”, “Repressors”, “Efforts to preserve the family”, “Inappropriate solving of family conflicts”, “Consequences”, and “Inefficient supportive systems” (Fig. 1 ).

Themes of domestic violence against women
Some of the statements of the participants on the theme of “ Facilitators” are listed below:
Husband’s criminal record
“He got his death sentence for drugs. But, at last it was ended for 10 years” (p 4, 54 yrs).
Inappropriate age for marriage
“At the age of thirteen, I married a boy who was 25 years old” (p 8, 25 yrs).
“My first husband obeyed her parents. I was 12–13 years old” (p 3, 32 yrs).
“I couldn’t do anything. I was humiliated” (p 1, 38 yrs).
“A bridegroom came. The mother was against. She said, I am young. My older sister is not married yet, but I was eager to get married. I don’t know, maybe my father’s house was boring for me” (p 2, 33 yrs).
“My parents used to argue badly. They blamed each other and I always wanted to run away from these arguments. I didn’t have the patience to talk to mom or dad and calm them down” (p 5, 39 yrs).
Overdependence
“My husband’s parents don’t stop interfering, but my husband doesn’t say anything because he is a student of his father. My husband is self-employed and works with his father on a truck” (p 8, 25 yrs).
“Every time I argue with my husband because of lack of money, my mother-in-law supported her son and brought him up very spoiled and lazy” (p 7, 55 yrs).
Bitter memories
“After three years, my mother married her friend with my uncle’s insistence and went to Shiraz. But, his condition was that she did not have the right to bring his daughter with her. In fact, my mother also got married out of necessity” (p 8, 25 yrs).
Some of their other statements related to “ Role failure” are mentioned below:
Lack of commitment to different roles
“I got angry several times and went to my father’s house because of my husband’s bad financial status and the fact that he doesn’t feel responsible to work and always says that he cannot find a job” (p 6, 48 yrs).
“I saw that he does not want to change in any way” (p 4, 54 yrs).
“No matter how kind I am, it does not work” (p 1, 38 yrs).
Some of their other statements regarding “ Repressors” are listed below:
Fear and silence
“My mother always forced me to continue living with my husband. Finally, my father had been poor. She all said that you didn’t listen to me when you wanted to get married, so you don’t have the right to get angry and come to me, I’m miserable enough” (p 2, 33 yrs).
“Because I suffered a lot in my first marital life. I was very humiliated. I said I would be fine with that. To be kind” (p1, 38 yrs).
“Well, I tell myself that he gets angry sometimes” (p 3, 32 yrs).
Shame from society
“I don’t want my daughter-in-law to know. She is not a relative” (p 4, 54 yrs).
Some of the statements of the participants regarding the theme of “ Efforts to preserve the family” are listed below:
Hope and trust
“I always hope in God and I am patient” (p 2, 33 yrs).
Efforts for children
“My divorce took a month. We got a divorce. I forgave my dowry and took my children instead” (p 2, 33 yrs).
Some of their other statements regarding the “ Inappropriate solving of family conflicts” are listed below:
Child-bearing thoughts
“My husband wanted to take me to a doctor to treat me. But my father-in-law refused and said that instead of doing this and spending money, marry again. Marriage in the clans was much easier than any other work” (p 8, 25 yrs).
Lack of effective communication
“I was nervous about him, but I didn’t say anything” (p 5, 39 yrs).
“Now I am satisfied with my life and thank God it is better to listen to people’s words. Now there is someone above me so that people don’t talk behind me” (p 2, 33 yrs).
Some of their other statements regarding the “ Consequences” are listed below:
Harm to children
“My eldest daughter, who was about 7–8 years old, behaved differently. Oh, I was angry. My children are mentally depressed and argue” (p 5, 39 yrs).
After divorce
“Even though I got a divorce, my mother and I came to a remote area due to the fear of what my family would say” (p 2, 33 yrs).
Social harm
“I work at a retirement center for living expenses” (p 2, 33 yrs).
“I had to go to clean the houses” (p 5, 39 yrs).
Non-acceptance in the family
“The children’s relationship with their father became bad. Because every time they saw their father sitting at home smoking, they got angry” (p 7, 55 yrs).
Emotional harm
“When I look back, I regret why I was not careful in my choice” (p 7, 55 yrs).
“I felt very bad. For being married to a man who is not bound by the family and is capricious” (p 9, 36 yrs).
Some of their other statements regarding “ Inefficient supportive systems” are listed below:
Inappropriate family support
“We didn’t have children. I was at my father’s house for about a month. After a month, when I came home, I saw that my husband had married again. I cried a lot that day. He said, God, I had to. I love you. My heart is broken, I have no one to share my words” (p 8, 25 yrs).
“My brother-in-law was like himself. His parents had also died. His sister did not listen at all” (p 4, 54 yrs).
“I didn’t have anyone and I was alone” (p 1, 38 yrs).
Inefficiency of social systems
“That day he argued with me, picked me up and threw me down some stairs in the middle of the yard. He came closer, sat on my stomach, grabbed my neck with both of his hands and wanted to strangle me. Until a long time later, I had kidney problems and my neck was bruised by her hand. Given that my aunt and her family were with us in a building, but she had no desire to testify and was afraid” (p 3, 32 yrs).
Undesired training and advice
“I told my mother, you just said no, how old I was? You never insisted on me and you didn’t listen to me that this man is not good for you” (p 9, 36 yrs).
Quantitative results
In the present study, 376 married women living in Semnan city participated in this study. The mean age of participants was 38.52 ± 10.38 years. The youngest participant was 18 and the oldest was 73 years old. The maximum age difference was 16 years. The years of marriage varied from one year to 40 years. Also, the number of children varied from no children to 7. The majority of them had 2 children (109, 29%). The sociodemographic characteristics of the participants are summarized in the table below (Table 3 ).
The frequency distribution (number and percentage) of the participants in terms of the level of violence was as follows. 89 participants (23.7%) had experienced low violence, 59 participants (15.7%) had experienced moderate violence, and 228 participants (60.6%) had experienced severe violence.
Cronbach’s alpha for the reliability of the questionnaire was 0.988. The mean and standard deviation of the total score of the questionnaire was 143.60 ± 74.70 with a range of 3-244. The relationship between the total score of the questionnaire and its fields, and some demographic variables is summarized in the table below (Table 4 ).
As shown in the table above, the variables of age, age difference and number of years of marriage have a positive and significant relationship, and the variable of number of children has a negative and significant relationship with the total score and all fields of the questionnaire (p < 0.05). However, the variable of education level difference showed no significant relationship with the total score and any of the fields. Also, the highest average score is related to patriarchal beliefs compared to other fields.
The comparison of the average total scores separately according to each variable showed the significant average difference in the variables of the previous marriage history of the woman, the result of the previous marriage of the woman, the education of the woman, the education of the man, the income of the woman, the income of the man, and the physical disease of the man (p < 0.05).
In the regression model, two variables remained in the final model, indicating the relationship between the variables and violence score and the importance of these two variables. An increase in women’s education and income level both independently show a significant relationship with an increase in violence score (Table 5 ).
The results of analysis of variance to compare the scores of each field of violence in the subgroups of the participants also showed that the experience and result of the woman’s previous marriage has a significant relationship with physical violence and tradition and family upbringing, the experience of the man’s previous marriage has a significant relationship with patriarchal belief, the education level of the woman has a significant relationship with all fields and the level of education of the man has a significant relationship with all fields except tradition and family upbringing (p < 0.05).
According to the results of both quantitative and qualitative studies, variables such as the young age of the woman and a large age difference are very important factors leading to an increase in violence. At a younger age, girls are afraid of the stigma of society and family, and being forced to remain silent can lead to an increase in domestic violence. As Gandhi et al. (2021) stated in their study in the same field, a lower marriage age leads to many vulnerabilities in women. Early marriage is a global problem associated with a wide range of health and social consequences, including violence for adolescent girls and women [ 12 ]. Also, Ahmadi et al. (2017) found similar findings, reporting a significant association among IPV and women age ≤ 40 years [ 19 ].
Two others categories of “Facilitators” in the present study were “Husband’s criminal record” and “Overdependence” which had a sub-category of “Forced cohabitation”. Ahmadi et al. (2017) reported in their population-based study in Iran that husband’s addiction and rented-householders have a significant association with IPV [ 19 ].
The patriarchal beliefs, which are rooted in the tradition and culture of society and family upbringing, scored the highest in relation to domestic violence in this study. On the other hand, in qualitative study, “Normalcy” of men’s anger and harassment of women in society is one of the “Repressors” of women to express violence. In the quantitative study, the increase in the women’s education and income level were predictors of the increase in violence. Although domestic violence is more common in some sections of society, women with a wide range of ages, different levels of education, and at different levels of society face this problem, most of which are not reported. Bukuluki et al. (2021) showed that women who agreed that it is good for a man to control his partner were more likely to experience physical violence [ 20 ].
Domestic violence leads to “Consequences” such as “Harm to children”, “Emotional harm”, “Social harm” to women and even “Non-acceptance in their own family”. Because divorce is a taboo in Iranian culture and the fear of humiliating women forces them to remain silent against domestic violence. Balsarkar (2021) stated that the fear of violence can prevent women from continuing their studies, working or exercising their political rights [ 8 ]. Also, Walker-Descarte et al. (2021) recognized domestic violence as a type of child maltreatment, and these abusive behaviors are associated with mental and physical health consequences [ 21 ].
On the other hand and based on the “Lack of effective communication” category, ignoring the role of the counselor in solving family conflicts and challenges in the life of couples in the present study was expressed by women with reasons such as lack of knowledge and family resistance to counseling. Several pathologies are needed to investigate increased domestic violence in situations such as during women’s pregnancy or infertility. Because the use of counseling for couples as a suitable solution should be considered along with their life challenges. Lin et al. (2022) stated that pregnant women were exposed to domestic violence for low birth weight in full term delivery. Spouse violence screening in the perinatal health care system should be considered important, especially for women who have had full-term low birth weight infants [ 22 ].
Also, lack of knowledge and low level of education have been found as other factors of violence in this study, which is very prominent in both qualitative and quantitative studies. Because the social systems and information about the existing laws should be followed properly in society to act as a deterrent. Psychological training and especially anger control and resilience skills during education at a younger age for girls and boys should be included in educational materials to determine the positive results in society in the long term. Manouchehri et al. (2022) stated that it seems necessary to train men about the negative impact of domestic violence on the current and future status of the family [ 23 ]. Balsarkar (2021) also stated that men and women who have not had the opportunity to question gender roles, attitudes and beliefs cannot change such things. Women who are unaware of their rights cannot claim. Governments and organizations cannot adequately address these issues without access to standards, guidelines and tools [ 8 ]. Machado et al. (2021) also stated that gender socialization reinforces gender inequalities and affects the behavior of men and women. So, highlighting this problem in different fields, especially in primary health care services, is a way to prevent IPV against women [ 24 ].
There was a sub-category of “Inefficiency of social systems” in the participants experiences. Perhaps the reason for this is due to insufficient education and knowledge, or fear of seeking help. Holmes et al. (2022) suggested the importance of ascertaining strategies to improve victims’ experiences with the court, especially when victims’ requests are not met, to increase future engagement with the system [ 25 ]. Sigurdsson (2019) revealed that despite high prevalence numbers, IPV is still a hidden and underdiagnosed problem and neither general practitioner nor our communities are as well prepared as they should be [ 26 ]. Moreira and Pinto da Costa (2021) found that while victims of domestic violence often agree with mandatory reporting, various concerns are still expressed by both victims and healthcare professionals that require further attention and resolution [ 27 ]. It appears that legal and ethical issues in this regard require comprehensive evaluation from the perspectives of victims, their families, healthcare workers, and legal experts. By doing so, better practical solutions can be found to address domestic violence, leading to a downward trend in its occurrence.
Some of the variables of violence against women have been identified and emphasized in many studies, highlighting the necessity of policymaking and social pathology in society to prevent and use operational plans to take action before their occurrence. Breaking the taboo of domestic violence and promoting divorce as a viable solution after counseling to receive objective results should be implemented seriously to minimize harm to women, children, and their families.
Limitations
Domestic violence against women is an important issue in Iranian society that women resist showing and expressing, making researchers take a long-term process of sampling in both qualitative and quantitative studies. The location of the interview and the women’s fear of their husbands finding out about their participation in this study have been other challenges of the researchers, which, of course, they attempted to minimize by fully respecting ethical considerations. Despite the researchers’ efforts, their personal and professional experiences, as well as the studies reviewed in the literature review section, may have influenced the study results.
Data Availability
Data and materials will be available upon email to the corresponding author.
Abbreviations
Intimate Partner Violence
Human Immunodeficiency Virus
Organization WH. Violence against women prevalence estimates, 2018: global, regional and national prevalence estimates for intimate partner violence against women and global and regional prevalence estimates for non-partner sexual violence against women. World Health Organization; 2021.
Huecker MR, Malik A, King KC, Smock W. Kentucky Domestic Violence. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Ahmad Malik declares no relevant financial relationships with ineligible companies. Disclosure: Kevin King declares no relevant financial relationships with ineligible companies. Disclosure: William Smock declares no relevant financial relationships with ineligible companies.: StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC.; 2023.
Gandhi A, Bhojani P, Balkawade N, Goswami S, Kotecha Munde B, Chugh A. Analysis of survey on violence against women and early marriage: Gyneaecologists’ perspective. J Obstet Gynecol India. 2021;71(Suppl 2):76–83.
Article Google Scholar
Sugg N. Intimate partner violence: prevalence, health consequences, and intervention. Med Clin. 2015;99(3):629–49.
Google Scholar
Abebe Abate B, Admassu Wossen B, Tilahun Degfie T. Determinants of intimate partner violence during pregnancy among married women in Abay Chomen district, western Ethiopia: a community based cross sectional study. BMC Womens Health. 2016;16(1):1–8.
Adineh H, Almasi Z, Rad M, Zareban I, Moghaddam A. Prevalence of domestic violence against women in Iran: a systematic review. Epidemiol (Sunnyvale). 2016;6(276):2161–11651000276.
Pirnia B, Pirnia F, Pirnia K. Honour killings and violence against women in Iran during the COVID-19 pandemic. The Lancet Psychiatry. 2020;7(10):e60.
Article PubMed PubMed Central Google Scholar
Balsarkar G. Summary of four recent studies on violence against women which obstetrician and gynaecologists should know. J Obstet Gynecol India. 2021;71:64–7.
Ellsberg M, Jansen HA, Heise L, Watts CH, Garcia-Moreno C. Intimate partner violence and women’s physical and mental health in the WHO multi-country study on women’s health and domestic violence: an observational study. The lancet. 2008;371(9619):1165–72.
Chasweka R, Chimwaza A, Maluwa A. Isn’t pregnancy supposed to be a joyful time? A cross-sectional study on the types of domestic violence women experience during pregnancy in Malawi. Malawi Med journal: J Med Association Malawi. 2018;30(3):191–6.
Afshari P, Tadayon M, Abedi P, Yazdizadeh S. Prevalence and related factors of postpartum depression among reproductive aged women in Ahvaz. Iran Health care women Int. 2020;41(3):255–65.
Article PubMed Google Scholar
Gebrezgi BH, Badi MB, Cherkose EA, Weldehaweria NB. Factors associated with intimate partner physical violence among women attending antenatal care in Shire Endaselassie town, Tigray, northern Ethiopia: a cross-sectional study, July 2015. Reproductive health. 2017;14:1–10.
Duran S, Eraslan ST. Violence against women: affecting factors and coping methods for women. J Pak Med Assoc. 2019;69(1):53–7.
PubMed Google Scholar
Devries KM, Mak JY, Garcia-Moreno C, Petzold M, Child JC, Falder G, et al. The global prevalence of intimate partner violence against women. Science. 2013;340(6140):1527–8.
Article CAS PubMed Google Scholar
Mahapatro M, Kumar A. Domestic violence, women’s health, and the sustainable development goals: integrating global targets, India’s national policies, and local responses. J Public Health Policy. 2021;42(2):298–309.
Lincoln YS, Guba EG. Naturalistic inquiry: sage; 1985.
Colaizzi PF. Psychological research as the phenomenologist views it. 1978.
Mohseni Tabrizi A, Kaldi A, Javadianzadeh M. The study of domestic violence in Marrid Women Addmitted to Yazd Legal Medicine Organization and Welfare Organization. Tolooebehdasht. 2013;11(3):11–24.
Ahmadi R, Soleimani R, Jalali MM, Yousefnezhad A, Roshandel Rad M, Eskandari A. Association of intimate partner violence with sociodemographic factors in married women: a population-based study in Iran. Psychol Health Med. 2017;22(7):834–44.
Bukuluki P, Kisaakye P, Wandiembe SP, Musuya T, Letiyo E, Bazira D. An examination of physical violence against women and its justification in development settings in Uganda. PLoS ONE. 2021;16(9):e0255281.
Article CAS PubMed PubMed Central Google Scholar
Walker-Descartes I, Mineo M, Condado LV, Agrawal N. Domestic violence and its Effects on Women, Children, and families. Pediatr Clin North Am. 2021;68(2):455–64.
Lin C-H, Lin W-S, Chang H-Y, Wu S-I. Domestic violence against pregnant women is a potential risk factor for low birthweight in full-term neonates: a population-based retrospective cohort study. PLoS ONE. 2022;17(12):e0279469.
Manouchehri E, Ghavami V, Larki M, Saeidi M, Latifnejad Roudsari R. Domestic violence experienced by women with multiple sclerosis: a study from the North-East of Iran. BMC Womens Health. 2022;22(1):1–14.
Machado DF, Castanheira ERL, Almeida MASd. Intersections between gender socialization and violence against women by the intimate partner. Ciência & Saúde Coletiva. 2021;26:5003–12.
Holmes SC, Maxwell CD, Cattaneo LB, Bellucci BA, Sullivan TP. Criminal Protection orders among women victims of intimate Partner violence: Women’s Experiences of Court decisions, processes, and their willingness to Engage with the system in the future. J interpers Violence. 2022;37(17–18):Np16253–np76.
Sigurdsson EL. Domestic violence-are we up to the task? Scand J Prim Health Care. 2019;37(2):143–4.
Moreira DN, Pinto da Costa M. Should domestic violence be or not a public crime? J Public Health. 2021;43(4):833–8.
Download references
Acknowledgements
The authors of this study appreciate the Deputy for Research and Technology of Semnan University of Medical Sciences, Social Determinants of Health Research Center of Semnan University of Medical Sciences and all the participants in this study.
Research deputy of Semnan University of Medical Sciences financially supported this project.
Author information
Authors and affiliations.
School of Allied Medical Sciences, Semnan University of Medical Sciences, Semnan, Iran
Mina Shayestefar & Mohadese Saffari
Amir Al Momenin Hospital, Social Security Organization, Ahvaz, Iran
Razieh Gholamhosseinzadeh
Department of Nursing, Faculty of Nursing and Midwifery, Semnan University of Medical Sciences, Semnan, Iran
Monir Nobahar
Social Determinants of Health Research Center, Semnan University of Medical Sciences, Semnan, Iran
Monir Nobahar & Majid Mirmohammadkhani
Clinical Research Development Unit, Kowsar Educational, Research and Therapeutic Hospital, Semnan University of Medical Sciences, Semnan, Iran
Seyed Hossein Shahcheragh
Student Research Committee, School of Allied Medical Sciences, Semnan University of Medical Sciences, Semnan, Iran
Zahra Khosravi
You can also search for this author in PubMed Google Scholar
Contributions
M.Sh. contributed to the first conception and design of this research; M.Sh., Z.Kh., M.S., R.Gh. and S.H.Sh. contributed to collect data; M.N. and M.Sh. contributed to the analysis of the qualitative data; M.M. and M.Sh. contributed to the analysis of the quantitative data; M.SH., M.N. and M.M. contributed to the interpretation of the data; M.Sh., M.S. and S.H.Sh. wrote the manuscript. M.Sh. prepared the final version of manuscript for submission. All authors reviewed the manuscript meticulously and approved it. All names of the authors were listed in the title page.
Corresponding author
Correspondence to Mina Shayestefar .
Ethics declarations
Ethics approval and consent to participate.
This article is resulted from a research approved by the Vice Chancellor for Research of Semnan University of Medical Sciences with ethics code of IR.SEMUMS.REC.1397.182 in the Social Determinants of Health Research Center. The authors confirmed that all methods were performed in accordance with the relevant guidelines and regulations. All participants accepted the participation in the present study. The researchers introduced themselves to the research units, explained the purpose of the research to them and then all participants signed the written informed consent. The research units were assured that the collected information was anonymous. The participant was informed that participating in the study was completely voluntary so that they can safely withdraw from the study at any time and also the availability of results upon their request.
Consent for publication
Not applicable.
Competing interests
All authors declare that there are no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Shayestefar, M., Saffari, M., Gholamhosseinzadeh, R. et al. A qualitative quantitative mixed methods study of domestic violence against women. BMC Women's Health 23 , 322 (2023). https://doi.org/10.1186/s12905-023-02483-0
Download citation
Received : 28 April 2023
Accepted : 14 June 2023
Published : 20 June 2023
DOI : https://doi.org/10.1186/s12905-023-02483-0
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Domestic violence
- Cross-sectional studies
- Qualitative research
BMC Women's Health
ISSN: 1472-6874
- Submission enquiries: [email protected]
- General enquiries: [email protected]

A.E. EYLER, M.D., M.P.H., AND MARIAN COHEN, A.C.S.W.
Am Fam Physician. 1999;60(9):2569-2576
A more recent article on the intimate partner violence is available .
See editorial on page 2498.
Interpersonal violence and abuse, especially between relatives and domestic partners, are leading causes of morbidity and mortality. Family physicians and other professionals who provide primary care health services must deal with acute presentations and chronic sequelae of this epidemic. Many victims of abuse hesitate to seek help, while those who batter are often difficult to identify. Medical management of patients in abusive relationships can be frustrating. Evaluating injury patterns, understanding factors that increase the risk for violence and making use of specific interview questions and techniques will aid family physicians in the difficult task of assessing and managing patients living in abusive partnerships.
The American Medical Association's Diagnostic and Treatment Guidelines on Domestic Violence state that, “Family violence usually results from the abuse of power or the domination and victimization of a physically less powerful person by a physically more powerful person.” 1 Other factors that create or maintain a power differential, such as unequal financial resources, family connections or health status, can also foster situations in which the more powerful person exerts inappropriate control or intimidation over the less powerful person. Any misuse of power, especially that which involves physical violence or psychologic intimidation, constitutes abuse. A perpetrator is a person who performs or permits the actions that constitute abuse or neglect. The term “batterer” refers more specifically to a perpetrator who engages in physical violence. It should be noted that, although the most familiar constellation for partner violence is one in which the (current or ex-) husband or boyfriend is the perpetrator and the wife or girlfriend is the victim, partner abuse also occurs in homosexual relationships and in heterosexual relationships in which men are the victims. Unless specifically mentioned, the remarks in this article are true for situations in which men and women are the abusers.
Although victimization is often dismissed as “human nature” (and therefore nonpreventable or remediable), cross-cultural research demonstrates that this is not the case. 2 Societies exist in which violence is rare and violence against women virtually nonexistent. Low-violence cultures share certain key characteristics that include strong sanctions against interpersonal violence, community support for victims, flexible gender roles for women and men, equality of decision-making and resources in the family, a cultural ethos that condemns violence as a means of resolving conflict, and female power and autonomy outside the home. 2 Table 1 lists factors that increase the likelihood that abuse and neglect may occur. These risk factors for abuse do not constitute “excuses” for violent behavior. They are presented as guidelines for early recognition and intervention by health professionals.
Medical Management Guidelines
General principles for the medical response to all forms of family violence are summarized in Table 2 . Clinical interventions specific to the problems of partner violence are discussed below in the context of two case presentations. Medical complications of partner abuse are listed in Table 3 .
Illustrative Cases
The following two cases, drawn from the clinical experiences of the authors, illustrate techniques for the diagnosis and management of patients experiencing interpersonal violence in partnered relationships. The discussion that follows each case is designed to assist family physicians with practical approaches to preventing violence and promoting victim safety.
An 18-year-old woman presented to her family physician for an initial obstetric examination, accompanied by her 27-year-old boyfriend. Initial history revealed that she was a gravida 1, para 0, at 16 weeks of gestation and living in a mobile home with her partner. She was strongly considering giving up the baby for adoption because of “financial and other” reasons. Answers to screening violence history questions ( Table 4 ) 1 indicated that she had been beaten by her father from preschool age until she was 13 years of age; her parents then divorced. The patient stated that her present partner had “slapped her around” on several occasions and that once she was “accidentally dragged by his truck” during an argument. He had slammed the driver's door, started the truck and put it in gear, reportedly without realizing that her dress was caught in the car door. On further questioning the patient stated that she was not happy in this relationship and in fact did not feel safe. However, she stated that she “had no place else to go”and expressed optimism about the future because her partner had begun to attend church and stated that he wanted to be a good father.
Battering is frequent during pregnancy 3 – 5 and is more common if, as in this case, the pregnancy is unintended. 6 Battering can result in pregnancy complications, delayed entry into prenatal care 7 , 8 and unintended, rapid-repeat pregnancy in adolescent mothers. 9 Simple screening questions, administered in a private setting, often identify pregnant women who are being abused. 7 Furthermore, because battering may begin late in pregnancy, a discussion of personal safety should be included at multiple times during the course of obstetric care.
This patient is a survivor of an abusive childhood. She lives with a partner who controls her behavior and who is on occasion physically abusive to her. She is also financially dependent on him. Her vulnerability is further increased, physically and psychologically, by her unplanned pregnancy and her lack of family or other emotional support.
Because battering usually does not abate during pregnancy, the physician can best intervene by providing her with information regarding the potential danger of her situation and by assisting her in safety planning, including a facilitated referral to a shelter for battered women. 10 One useful technique is for the physician to contact the shelter while the patient is in the examination room or a private office. The physician can then hand the telephone to the patient and leave the room, allowing the patient to talk to a counselor in private. Thus, the patient's autonomy and privacy are respected, but an additional barrier to seeking help is removed.
The physician should inquire about the presence of firearms in the home or in the possession of the battering partner. This step is crucial in preventing serious injury and homicide. 11 – 13 Statistics from the Federal Bureau of Investigation indicate that over one half of female murder victims are killed by firearms in the hands of a current male partner or ex-husband.
It is also crucial that, throughout the course of the pregnancy, the physician avoid communicating to the patient that she is in any way responsible for, or deserving of, the abuse. 14 For example, asking her why she is still living with her partner may be interpreted as a judgment of her failure to end the relationship. Furthermore, as most men who batter will from time to time express goodwill or intent to change, it may be helpful to ask the patient if her partner has previously made promises of improved behavior and inquire if he has kept such promises. The physician may wish to review the elements of abuse outlined in Table 5 with the patient and ask about her partner's behaviors. This table illustrates the many faces of abuse and may help her visualize and assess her risk in light of the overall circumstances, rather than focusing on her partner's latest promises. She may be unaware that the main issues in abusive relationships are power and control.
Many batterers who eventually stop using physical violence substitute psychologic abuse and intimidation. 15 Thus, it may further help the patient to understand that even in relationships in which the physical violence has ceased, a climate of fear may persist to a level where the formerly battered partner continues to comply with the requests of the dominant partner out of fear that the physical violence will resume.
When discussing postpartum contraception with women living in an abusive partnership, it is important for the physician to bear in mind that such relationships often include forced or coercive intercourse. The family physician should ask the patient about unwanted sexual contact, even if the patient is married or living with an intimate partner. Some abusers sabotage contraceptive efforts (i.e., steal oral contraceptives or refuse to use condoms) in order to maintain control in the relationship. If the patient does not leave the abusive partner, these issues must be discussed. A non-coitus–dependent contraceptive method, such as progesterone implants (Norplant), may be the best option. 9
This abusive relationship was detected through the routine application of questions screening for violence risk in intimate partnerships ( Table 4 ) . 1 Other signs that often indicate a need to further assess the risk of abuse include excessive work loss, sleep disturbances, substance abuse, somatization or “bad nerves,” sexual dysfunction, depression, frequent injuries or being “accident prone.” 16 In this case, it is extremely important to review any records received from emergency departments, urgent care facilities and any obstetric colleagues (e.g., cross-coverage providers) during the remainder of her pregnancy and postpartum period. It is imperative to discuss events noted in these records with the patient and to assess any discrepancy between an injury and its reported causative mechanism, because injuries related to battering are often attributed to falling on the stairs or some other household accident. In such cases, the patient should be asked to describe the accident in more detail, or the physician should ask about precipitating factors (e.g. “were you pushed?”). Ancillary tests should be obtained as indicated for the specific injury or infection. The physician should be especially alert for pregnancy complications and sexually transmitted infections, including human immunodeficiency virus infection.
Factors that specifically relate to partner abuse include the following: (1) a power differential in the relationship in which one partner is financially or emotionally dependent on the other; (2) a temporary or permanent disability (including pregnancy); (3) a force orientation—a belief on the part of the perpetrator that violence is an acceptable solution to conflicts and problems, and (4) a personal or family history of abuse. It may be useful to ask the patient how her partner manages frustration or stress. Does he blame others (including her) or does he take responsibility for his mistakes? Does he use aggression (including threats or put-downs) to resolve conflicts in the relationship?
A 45-year-old man presented to his physician with a complaint of worsening depression. The patient had been taking antidepressant medications for many years, was receiving ongoing psychotherapy from a clinical social worker and attending Alcoholics Anonymous meetings. The patient complained of insomnia, loss of appetite and thoughts of guilt and suicide since his spouse had “kicked him out.” He was especially concerned because she has multiple sclerosis, relies on him for some physical assistance and, in his opinion, should not be left alone. Further discussion revealed that during an argument, he verbally threatened to harm her, then threw a large lamp at her (although he missed and did not actually hit her). She called the police, had him removed from the home and told him she would soon be filing for divorce.
A positive outcome is possible for this couple because of the confluence of several helpful events and interventions. The patient had previously received treatment for alcoholism, had not resumed drinking and was under care for depression. Furthermore, his wife had worked as a teacher before her illness, was receiving retirement benefits and was not financially dependent on him. Perhaps most significantly, she called the police during the first violent episode rather than excuse her husband's actions and allow a pattern of threats and intimidation to become established. She also received a prompt response and support from the police and the courts.
The patient's depression worsened during the court proceedings, eventually requiring inpatient psychiatric treatment for suicide prevention. During the course of his therapy, he received psychologic support for his stressful personal situation, but his behavior toward his wife was not excused in any way by his treating physicians. Eventually, this couple began marital therapy together, after the goals of establishing a non-violent and equitable relationship were defined.
Family physicians can play a crucial role in referring batterers to appropriate services for behavior modification interventions and treatment of comorbidities, such as depression and alcoholism. If the abusive patient's wife or partner is also a patient in the physician's practice, asking that person questions about her experiences of violence and providing information about safety planning and resources may be lifesaving. 10 , 17
Studies have not identified any consistent psychiatric diagnoses among batterers, but abusive men share some common characteristics such as rigid sex-role stereotypes, low self-esteem, depression, a high need for power and control, a tendency to minimize and deny their problems or the extent of their violence, a tendency to blame others for their behavior, violence in the family of origin (particularly witnessing parental violence), and drug and alcohol abuse (which are not causative but are often associated). 18 Some but not all batterers meet the criteria in the Diagnostic and Statistical Manual of Mental Disorders , 4th ed. (DSM–IV) for personality disorders or depression. 19
Men who have alcoholism combined with a major depressive disorder or antisocial personality disorder are more likely to commit domestic violence than men with either of these conditions alone. 20 Most researchers believe that abusive behavior is the result of multiple factors, including individual characteristics, a family history of violence, the culturally rooted belief that violence is an acceptable means of solving problems and that violence toward women is acceptable or tolerated. 21 , 22 The patient in this case did not hold these beliefs and was eventually able to participate successfully in couples' therapy.
Batterers are often difficult to identify because they rarely present with symptoms that suggest problems with violence; however, they may seek care for injuries received from a violent episode where the victim's attempts at self-defense result in injuries to the batterer (e.g., hand fractures, bites, lacerations, eye injuries).
Family physicians can also screen for violent behavior by asking direct questions 23 or by inquiring about related beliefs and behaviors while conducting a routine patient history. One such approach is the funneling technique ( Table 6 ) , which begins with less threatening questions and progresses to questions about more serious violence, depending on the patient's responses. Batterers often minimize or deny their abuse by using euphemisms for violence such as “not getting along,” “loss of temper,” “fighting” and “self-defense,” when in fact they are referring to their own violent actions. 15 Therefore, questioning does not always result in identification of battering behavior. Nevertheless, this approach allows the physician to broach the subject, and further questioning about what the patient means by a specific term may sometimes provide the opportunity for the patient to disclose abusive actions and seek help.
Patients who batter should be advised that their behavior is illegal and should be given information about treatment programs. Family physicians should bear in mind that the usefulness of batterer treatment programs remains controversial. 24 Many perpetrators do not change their beliefs or behavior, and the immediate goal is protection of the battered patient and dependents (children and elderly relatives) from further harm. Early referral to community resources (e.g., safe houses and legal aid) and follow-up until the situation is resolved can be crucial. Encouraging the battered victim to call the police or involve sympathetic family members or friends may help alleviate the isolation that often accompanies domestic violence and also help prevent retaliation.
In this case, the patient's wife was able to make use of multiple sources of support to remain safe in her own home during her partner's arrest, brief incarceration and treatment. She was also fortunate in that he recognized his behavior as problematic and genuinely wished to change. Most situations involving partner violence are not as amenable to a positive outcome. In many cases, the victimized partner remains in danger for years. Couples' therapy should not be attempted until it is clear that the violence has stopped and the perpetrator has undergone successful treatment. 15 Physicians may inadvertently collude with the batterer by encouraging a premature reunion of the couple.
The simultaneous actions of medical, mental health and law enforcement personnel, plus the determination of this couple, resulted in a positive outcome. Nonetheless, family physicians should remain aware that, without adequate community support from the police and courts, outcomes such as this one are rare.
All intervention should be conducted in a supportive atmosphere with confidentiality assured. The physician should ask the patient if it is safe to take home written materials that pertain to domestic violence. If not, important telephone numbers can be offered on plain stationery or a prescription sheet. As part of a safety plan, the physician should arrange for a safe way to follow-up with the patient by telephone. For example, if a call from the medical office might arouse the suspicions of the batterer, the physician and patient could agree in advance to say that the call was from a local business. Physicians may wish to ask the patient ahead of time for the name of a friend who can be contacted as a way of reaching the patient, if necessary. The patient should be asked if the physician can call the police if he or she is unable to contact the patient and believes the patient might be in immediate danger.
Occasional conflict is a universal feature of intimate relationships. However, coercion, violence and unwanted sexual activity are not a normal part of marriage or other relationships and must not be tolerated. Many alternatives exist for handling conflict that do not involve violence, intimidation or domination of one person by the other. Prevention of abuse and neglect depends on the early recognition of risk and on timely, appropriate response.
Physicians frequently report that dealing with domestic violence is a frustrating experience. Persons who have been abused are often not “ideal” patients—they miss appointments, request tranquilizers, offer vague somatic complaints, do not follow through with treatment and often do not leave their batterers.
In contrast, perpetrators are often articulate, interesting community figures who present themselves more favorably. 17 In order to deal most effectively with the problem of partner abuse and to maintain a balanced perspective, family physicians must remain aware that appearances can be deceiving. Incorporating routine screening for violence risk into clinical practice may minimize the risk that a physician will fall prey to unconscious stereotypes about abused persons.
Domestic violence is a criminal offense. Patient education about these straightforward facts, during office visits or through written materials and timely referral, can be lifesaving. Resources are listed in Table 7 .
Final Comment
Family physicians can prevent suffering, serious injury and death by remaining alert to the possibility of interpersonal violence and victimization when evaluating health risks during routine practice. Early intervention, including timely legal involvement and emergency service provision, in a context of community support, may prevent further violence and later sequelae. In addition, efforts by family physicians and other concerned persons to increase societal awareness of the problem of violence, to highlight the unacceptability of interpersonal violence as a means of resolving conflict and to provide alternative strategies for dealing with frustration in family relationships may eventually decrease the incidence of domestic abuse and its medical complications.
Flitcraft AH, Hadley SM, Hendricks-Matthews MK, McLeer SV, Warshaw C, et al. Diagnostic and treatment guidelines on domestic violence. Chicago: American Medical Association, 1992.
Heise LL. Gender-based abuse: the global epidemic. In: Dan AJ, ed. Reframing women's health: multidisciplinary research and practice. Thousand Oaks, Calif.: Sage Publications, 1994:233–50.
Gazmararian JA, Lazorick S, Spitz AM, Ballard TJ, Saltzman LE, Marks JS. Prevalence of violence against pregnant women. JAMA. 1996;275:1915-20.
McFarlane J, Parker B, Soeken K. Abuse during pregnancy: associations with maternal health and infant birth weight. Nurs Res. 1996;45:37-42.
Physical violence during the 12 months preceding childbirth—Alaska, Maine, Oklahoma, and West Virginia, 1990–1991. MMWR Morb Mortal Wkly Rep. 1994;43(8):132-7.
Gazmararian JA, Adams MM, Saltzman LE, Johnson CH, Bruce FC, Marks JS, et al. The relationship between pregnancy intendedness and physical violence in mothers of newborns. The PRAMS Working Group. Obstet Gynecol. 1995;85:1031-8.
McFarlane J, Parker B, Soeken K, Bullock L. Assessing for abuse during pregnancy. Severity and frequency of injuries and associated entry into prenatal care. JAMA. 1992;267:3176-8.
Dietz PM, Gazmararian JA, Goodwin MM, Bruce FC, Johnson CH, Rochat RW. Delayed entry into prenatal care. Obstet Gynecol. 1997;90:221-4.
Jacoby M, Gorenflo D, Black E, Wunderlich C, Eyler AE. Rapid repeat pregnancy and experiences of interpersonal violence among low-income adolescents. Am J Prev Med. 1999;16:318-21.
McFarlane J, Soeken K, Reel S, Parker B, Silva C. Resource use by abused women following an intervention program: associated severity of abuse and reports of abuse ending. Public Health Nurs. 1997;14:244-50.
McFarlane J, Parker B, Soeken K. Abuse during pregnancy: frequency, severity, perpetrator, and risk factors of homicide. Public Health Nurs. 1995;12:284-9.
McFarlane J, Soeken K, Campbell J, Parker B, Reel S, Silva C. Severity of abuse to pregnant women and associated gun access of the perpetrator. Public Health Nurs. 1998;15:201-6.
Saltzman LE, Mercy JA, O'Carroll PW, Rosenberg ML, Rhodes PH. Weapon involvement and injury outcome in family and intimate assaults. JAMA. 1992;267:3043-7.
Hamberger LK, Ambuel B, Marbella A, Donze J. Physician interaction with battered women. 1998;7:575-82.
Adams D. Guidelines for doctors on identifying and helping their patients who batter. J Am Med Womens Assoc. 1996;51:123-6.
Sassetti MR. Battered woman. In: Violence education: toward a solution. Hendricks-Matthews MK, Brewster A, eds. Kansas City, Mo.: Society of Teachers of Family Medicine, 1992:31–9.
Ferris LE, Norton PG, Dunn EV, Gort EH, Degani N. Guidelines for managing domestic abuse when male and female partners are patients of the same physician. The Delphi Panel and the Consulting Group. JAMA. 1997;278:851-7.
Bennett LW. Substance abuse and the domestic assault of women. So Work. 1995;40:760-71.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, D.C.: American Psychiatric Association, 1994:317–92.
Keller LE. Invisible victims: battered women in psychiatric and medical emergency rooms. Bull Menninger Clinic. 1996;60:1-21.
Chell D. Who are the batterers?. Iowa Med. 1995;85:28-30.
Hamberger LK. Identifying and intervening with men who batter. In: Hendricks-Matthews MK, Brewster A. Violence education: toward a solution. Kansas City, Mo.: Society of Teachers of Family Medicine, 1992:55–62.
Oriel KA, Fleming MF. Screening men for partner violence in a primary care setting. J Fam Pract. 1998;46:493-8.
Tolman R, Edleson J. Intervention for men who batter: a review of research. In: Stith SM, Straus MA, eds. Understanding partner violence: prevalence, causes, consequences, and solutions. Minneapolis, Minn.: National Council on Family Relations 1995:262–74.
Continue Reading
More in afp, more in pubmed.
Copyright © 1999 by the American Academy of Family Physicians.
This content is owned by the AAFP. A person viewing it online may make one printout of the material and may use that printout only for his or her personal, non-commercial reference. This material may not otherwise be downloaded, copied, printed, stored, transmitted or reproduced in any medium, whether now known or later invented, except as authorized in writing by the AAFP. See permissions for copyright questions and/or permission requests.
Copyright © 2024 American Academy of Family Physicians. All Rights Reserved.
Academia.edu no longer supports Internet Explorer.
To browse Academia.edu and the wider internet faster and more securely, please take a few seconds to upgrade your browser .
Enter the email address you signed up with and we'll email you a reset link.
- We're Hiring!
- Help Center

Case study: Domestic Violence and Trauma

Josie (25) is referred to you by her GP for depression. She lives with her husband (Greg, 27) and children (aged 2 and 4). She says she is not coping. She thinks she’s going to get the sack from her part-time job because she’s missed a few days “when the kids were sick”. Her husband works long hours and often gets stressed and shouts at her or the children. However, she denies any physical abuse. She likes her job but it is difficult with the children as she has no family support – her father was physically abusive and left the family when she was 13 and she avoids her mother because she is “a sad alcoholic”. Her only sibling (Mary) “escaped” from home when she turned 18 and Josie has lost contact with her. She sometimes has flashbacks and nightmares about her childhood. Josie works as a mental health support worker and would like to pursue further studies when the children start school. 1) What other questions would you want to include in your assessment and why? 2) Present a case formulation and discuss evidence based theories underpinning your formulation and also interventions. 3) Discuss ways in which you would assist your client to deal with some of the legacies of trauma. You are welcome to introduce an integrative approach but you need to make sure that your interventions are cohesive and “make sense” to the client and your view of trauma treatment. 4) Discuss possible roadblocks in therapy and how you plan to address them
Related Papers
Journal of Emotional Abuse
Anna Fairtlough
The Department of Health publication, Commissioning services for women and children who have experienced violence or abuse – a guide for health commissioners, clearly acknowledges that ‘victims of violence or abuse tend to use health services more than average’ and that this is ‘despite often finding it hard to access services’ (Golding and Duggal, 2011: 22). The guidance goes on to state that it is precisely because of this that ‘it is in the NHS interest to identify these women and children, provide opportunities for them to disclose, and provide services [..] to help them improve their physical and mental health’ (ibid). The policy that has been implemented to support this process is known as ‘routine enquiry’ (RE). Since 2003 it has been Department of Health policy that all adult service users should be asked about experiences of violence and abuse in mental health assessments. However, asking about experiences of abuse and violence is not enough. To be effective the policy of r...
Child & Family Social Work
Sass Boucher
Family Practice
Nicky Stanley
Professional Psychology: Research and Practice
Christine A. Courtois
margarita Frederico
Child Care in Practice
Stephen Coulter
The focus of this paper is on the author's multi-modal therapeutic practice with a 7-year-old boy referred to the Family Trauma Centre, following paramilitary assaults on his father. The work also addresses the boy's experience of domestic violence. ... The work is contextualised ...
Roxane Agnew-davies
BJPsych bulletin
Pallab Majumder
RELATED PAPERS
Professor Indra Abeysekera
Human Reproduction
Ismail Acar
Revue Géographique de l'Est
Julien Aimé
arXiv: Mathematical Physics
Carlos Mora González
Monica Chavez
Journal of Comparative Neurology
Gabriel Real Ferrer
Jurnal HIDROPILAR
johar setiyadi
Natura@economía
Manuel Ego-Aguirre
Athanasia Petala
Physical Review Letters
shannon watson
Carla Calixto
Prince Gupta
Enciclopédia Biosfera
amintas rossete
Ademar Romeiro
Digestive diseases and sciences
Trầm Bảo Trân
Nature Genetics
Mohsen Khademi
Journal of Cardiac Surgery
Tamiyuki Obayashi
办莫纳什大学Monash毕业证书 澳洲大学文凭学历证书
Microorganisms
Joseph Djaman
Journal of Shoulder and Elbow Surgery
john zavala
特拉华大学毕业证成绩单 特拉华大学文凭学历证书哪里能买
The British journal of general practice : the journal of the Royal College of General Practitioners
Ahmed Rashid
call girls delhi
RELATED TOPICS
- We're Hiring!
- Help Center
- Find new research papers in:
- Health Sciences
- Earth Sciences
- Cognitive Science
- Mathematics
- Computer Science
- Academia ©2024

Local news, paywall-free.
MinnPost’s timely reporting is available for free, all year round. But our work isn’t free to produce. Support our nonprofit newsroom with a tax-deductible donation today.
Nonprofit, independent journalism. Supported by readers.
University of Minnesota studies reveal disparities in intimate partner violence between rural and urban areas
Share this:.
- Click to email a link to a friend (Opens in new window)
- Click to share on Facebook (Opens in new window)
- Click to share on Twitter (Opens in new window)
- Click to print (Opens in new window)

Domestic abuse involving intimate partners is happening at a higher rate in the nation’s rural areas than it is in urban ones, a problem made worse by fewer safety screenings of people who are potentially at risk for abuse, according to studies conducted by a team of researchers at the University of Minnesota.
One of the studies, conducted through the university’s Rural Health Research Center , looked at the challenges faced by victims and survivors of such violence in rural areas. It did so by speaking with advocacy organizations, state-based coalitions and service organizations that help victims of intimate partner violence.
Other studies found that physical intimate partner violence is more common among rural expectant mothers in the U.S. and that rural victims of intimate partner violence are at a higher risk of not being screened for abuse compared with those in urban areas. The researchers hope their work will shed light on the extent of domestic partner violence in rural spaces, which some say are ill-equipped to deal with the trend because they are underfunded and understaffed.
The team interviewed staff members from 15 organizations, including five national policy and advocacy service groups, five state-based coalitions and five direct service organizations that serve rural communities in four states. The Minnesota organizations included Violence Free Minnesota, the Minnesota Indian Women’s Resource Center and Southwest Crisis Center.
Challenges for rural victims
Many of the groups brought up similar themes that pose challenges for the prevention of intimate partner violence, said Alyssa Fritz, a research and policy fellow of the Rural Health Research Center and co-author of the studies.
Mandated reporting laws, for example, can often result in negative impacts for the victim, said Guadalupe Lopez, the executive director of Violence Free Minnesota, a statewide coalition of organizations that work to end relationship abuse.
Lopez has seen children separated from their mothers and removed from their homes because abuse was reported.
“Someone that is experiencing violence already has a loss of control or power over their life and loss of agency and so having this decision made for them … it’s another way of taking away some of that power,” Fritz said.
Interviewees who talked to Fritz also shared the importance of sexual assault nurse examiners (SANE). Those nurses have additional training that helps them care for sexual assault victims — and have been shown to improve health outcomes. Lopez said they are “incredibly important” to communities but that there’s also a need for nurses who know how to deal with domestic violence cases and collect forensic evidence.
Fritz said many organizations expressed a shortage of SANE nurses in rural areas. A study of the availability of SANE practitioners in Pennsylvania, for instance, found that in 2022 only 16.7% of rural Pennsylvania counties had a certified SANE, compared with 68.4% of nonrural counties.
Higher rates of partner violence
The University of Minnesota’s research found that nationwide, 4.6% of rural residents and 3.2% of urban residents reported experiencing physical violence from a current or former intimate partner.
Greater Minnesota is also overrepresented in intimate partner homicides based on its smaller population. A report from Violence Free Minnesota found that from 1989 to 2018, 45.5% of intimate partner homicides of women were in Greater Minnesota and 54.5% were in the metro.
“A lot of people have the stereotype that inner city and urban areas carry the most violence,” Lopez said.
Lopez said some communities don’t hold people accountable in the same ways as others.
“Each county, each city handles domestic violence so differently,” she said. “Some cities have domestic violence courts that really pay attention and hold that violence in a different way, and some cities don’t, where things are falling through the cracks.”
Much of the university’s research focuses on potential solutions that could help victims when they’re facing intimate partner violence. Some organizations brought up financial help for victims as a key pathway.
“Not being able to support oneself is one of the top reasons that victims feel like they can’t leave abusive situations,” Fritz said. “People know their needs more than anyone else.”
Oregon, for example, offers temporary funds to domestic violence survivors.
Meggie Royer, the prevention program manager at Violence Free Minnesota, said the staffing and the funding of shelters and other forms of support is a concern in rural areas because often one office is the only resource available.
In rural areas, Royer said transportation to a shelter or community organization that offers aid is also a barrier to receiving help.
Fewer screenings in rural areas
The research also found that victims of partner abuse in rural areas were less likely to be asked about abuse in healthcare settings, which could provide a chance for intervention.
Before pregnancy, 60.4% of rural residents and 57.8% of urban residents who experienced intimate partner violence were not screened for abuse, according to the research. Many of the victims lacked health care visits before pregnancy, with approximately 35% of rural residents and 33.1% of urban residents who experienced intimate partner violence not having attended a visit in the year before their pregnancy.
The research found that 21.3% of rural residents and 16.5% of urban residents who experienced intimate partner violence reported not receiving abuse screening. In addition, 40% of rural and 36.3% of urban victims were not screened at the visits they did attend, which Fritz found alarming. “Healthcare is such an important place to have to be screened or have resources,” Fritz said. “For some people, it might be the only confidential place they can access support for it.”

Ava Kian Ava Kian is MinnPost’s Greater Minnesota reporter. Follow her on Twitter @kian_ava or email her at [email protected] .
Thanks to our major sponsors

We've recently sent you an authentication link. Please, check your inbox!
Sign in with a password below, or sign in using your email .
Get a code sent to your email to sign in, or sign in using a password .
Enter the code you received via email to sign in, or sign in using a password .
Subscribe to our newsletters:
- Daily Newsletter MinnPost's top stories delivered to your inbox Monday through Saturday.
- Events & member benefits Be the first to know about opportunities around MinnPost membership & events.
Sign in with your email
Lost your password?
Try a different email
Send another code
Sign in with a password
Privacy Policy
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
Case Study: Intimate Partner Violence
Rebecca Plett, PhD
Sarah is having her first baby. She’s in her early 20s, and recently married: her parents and in-laws spent a lot of money on a lavish church wedding and honeymoon. On her wedding day, Sarah paused on her way into the church, her arm linked in her father’s, feeling a dread in her gut that she was making the wrong decision in marrying this man but currently saw no way out; few narratives had shown her a life other than marriage to a man and children.
Several years earlier, after high school, Sarah got a job at a factory. There she noticed a young man paying particular attention to her, someone known around the factory as a nice guy, and she decided to go on a date with him, not having had any previous romantic encounters. The date started off well, and after dinner and a movie, he offered to drive her home. Instead of taking her straight there, however, he took Sarah to a secluded area and demanded she have sex with him. When she said no, he did anyway, forcibly. After a derogatory comment about her loss of virginity, he dropped her off at her parent’s home. Feeling overwhelmingly ashamed and shocked, Sarah took a bath and contemplated taking a bottle of pills. The next day, she told her mother what happened, and her mother, fearing her daughter be labelled as promiscuous, urged that Sarah marry him and make the best of the situation.
Caring deeply about her family’s approval, Sarah got married despite a sense of dread. She became pregnant shortly after her wedding, and her husband also began hitting her around this time. Feeling an overwhelming instinct to protect her child, Sarah did everything in her power to placate her husband, including enabling his drinking to the point he would pass out and would no longer be a threat. Throughout her pregnancy, her husband became increasingly violent, though he avoided causing visible evidence, and became obsessed with the possibility that this wasn’t his child, and that Sarah had cheated on him.
Of course, you don’t know any of this when you meet Sarah for the first time. What you do notice is that she has a slight bruise around her wrist, and her husband hasn’t come to any appointments: a fact that Sarah defends with vigour. You begin to suspect she might not be safe, and are also concerned for what may transpire when the baby comes.
What are some of your options in seeing Sarah through her pregnancy and labour with care?
a) During one of your appointments, you could confront Sarah directly and tell her she needs to leave her husband. b) You could call the police, or the local child-and-family services (at this point, there are no children involved). c) You could build trust with Sarah for a few appointments by supporting her and being positive about her. d) Be indirect in offering resources and support services
While you may feel a sense of urgency in assuring Sarah and her child’s safety, answers a) and b) have the potential to make matters worse for her. Here are a few things to keep in mind when caring for a client who appears to be in a situation of partner violence:
- Clients with abusive partners may experience the most abuse during the pregnancy and postpartum periods (Moore 1999); Expectant fatherhood can arouse feelings of fear and insecurity in the father-to-be about his own role in parenting, especially if he faced abuse from his own father. These feelings can manifest through control and abuse of partners. In Sarah’s case, her husband was abused by his father.
- Often, abusive partners maintain control through emotional and psychological violence, making it less visible. Sarah’s husband, for instance, has repeated told her she is “ruined” for any other man, and that he is the only one who will “put up” with her. Because of this, Sarah feels the unbearable tension of being afraid of leaving, and ashamed that she stays.
- Direct confrontation – saying “you need to leave right now,” for instance – can potentially increase danger. Sometimes criticism of abusive partners can lead to the client becoming defensive of their partner and their situation, particularly if the direction makes them feel ashamed of staying in a situation they know is dangerous, but can’t yet leave.
- Depending on the situation, some abusers exert control by requiring their partners to report every interaction with every person they encounter. For instance, after a midwifery appointment, the client may feel they need to report what was discussed, and if the midwife recommended leaving, this may lead to anger by the abusive partner that puts the client in significant danger. In addition, further controls may be put on the client (like not being able to go out at all), narrowing their scope of support.
- Leaving a violent relationship is not simple, and a safety plan needs to be in place before someone may decide leaving is better than staying (Macy et al. 2009). These plans can include securing a safe place to go, like a relative’s house or shelter; keeping important documents in a hidden location; memorizing emergency numbers, and assuring financial security. Sarah’s husband controls their bank accounts, but she has been reserving small amounts of cash when he asks her to take out money for his trips to the bar.
- Violence often leads to chronic health problems, which can impede the ability of carry out a safety plan. (Macy et al. 2009) During pregnancy, the development of chronic conditions due to physical violence increases stress, creates delays in seeking care, and can lead to poor nutrition, and substance abuse to cope (Moore 1999).
- Those in situations of violence are not passive victims, but are often weighing their options carefully: Sarah, for example, knows she shouldn’t be ‘letting’ this happen to her, but is anxious about her ability to care for a new baby on her own, her financial well-being if she leaves, and her family’s insistence that divorce is a sin. These may seem to be trivial, but for Sarah, these are her very real struggles, and it is because of this that many prefer the term survivor over victim.
What can you do as a midwife?
- Screening for violence should be universal; that is, all clients can be given information on resources and safety – this also needs to be done apart from partner
- Providing information for leaving an abusive relationship (how to develop a safety plan, signs of violence, expectations of what a healthy relationship looks like, and resources available (like shelters, financial and legal aid)) can be done anonymously through posters in offices, bathrooms, exam rooms, and brochures given directly. Even providing ‘safety cards’ throughout the clinic that are discreet and carry useful information about resources.
- When leaving a violent situation, many clients need the support of a variety of services. Midwives can foster a sense of community practice and advocacy by familiarizing themselves with the services available – counselling, legal and financial aid, medical services beyond birth care, housing, etc.
- Ultimately, those in violent situations need support in a non-judgemental setting: you should be there to offer a relationship built on trust and support, to build the client up and emphasize the positive aspects of what they are doing in relation to their pregnancy, birth, and care of their infant. In this way, you can say in a context of trust, “when you’re ready, here are some resources and supports that you can access in order to help you leave.”
Case Study: Intimate Partner Violence Copyright © 2017 by Rebecca Plett, PhD is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License , except where otherwise noted.
Share This Book
IMAGES
VIDEO
COMMENTS
Domestic Violence. Using Law and Leaving Domestic Violence. The following case studies are based on interviews undertaken with women who agreed to be interviewed as part of the Using Law and Leaving Domesic Violence research project. In order to maintain the anonymity of the participants some information has been removed.
A case study of the impacts of domestic and family violence on women and their children This case study is drawn from one of the interview participants in the 'Domestic and family violence and parenting: Mixed method insights into impact and support needs' research report led by Dr Rae Kaspiew and published by ANROWS.
Ravi went to Criminal Court in May 2018 where he pleaded guilty to the charges. Sonali was fearful for her life and sought a restraining order . As a result of the abuse, Sonali developed anxiety, constantly feels stressed, and has difficulty concentrating. She has trust issues and difficulties forming relationships.
— Executive summary of the Report of the Special Rapporteur on Violence against Women,1 6 January 2003 iv INTRODUCTION 1 United Nations document E/CN.4/2003/75. 2 A note on terminology: We are using the term 'violence against women' rather than 'gender-based violence' since this study is looking only at violence against women and girls.
24 November 2021 Women. Conflicts, humanitarian crises and increasing climate-related disasters have led to higher levels of violence against women and girls (VAWG), which has only intensified during the COVID-19 pandemic, bringing into sharp focus the urgent need to stem the scourge. Globally, nearly one-in-three women have experienced ...
In a case study of two boys (aged 12 and 13; Dryden et al., 2010), the "heroic protection discourse" (HPD) is utilized to explore gendered understandings of violence. HPD refers to: "…a set of interpretative resources and practices that normalize a form of masculine identity that combines physical strength and aggression with the ...
Book Information. "Domestic Violence in Immigrant Communities: Case Studies" is a freely accessible eCampus Ontario Pressbook containing case studies of immigrant women experiencing domestic violence to be used as educational materials. The contents were created by analysing closed legal case files of 15 immigrant women living in Ontario ...
The Domestic Violence Evidence Project (DVEP) is a multi-faceted, multi-year and highly collaborative effort designed to assist state coalitions, local domestic violence programs, researchers, and other allied individuals and organizations better respond to the growing emphasis on identifying and integrating evidence-based practice into their work. . DVEP brings together research, evaluation ...
Ramandeep agreed reluctantly and the son was sent to India for two years. The verbal and physical abuse continued, and Aman demanded sex daily. Their son returned to Canada two years later in May 2009. Both children, at this point, had witnessed much violence over the years and were afraid of their father and would hide from him.
This study explores women and their children's lived experience of domestic violence (DV). A qualitative phenomenological research approach was used. Data were collected by semi-structured ...
The Domestic Violence Power and Control Wheel-Developed by: Domestic Abuse Intervention Project. ... While SWHTF is a relevant example, the focus of this case study is the project conducted with Fort Bend Women's Center (FBWC). We found the most effective approach to building trust and understanding was to focus on educating staff about our ...
Women's Aid have a checklist that can help you identify if you are in an abusive relationship. View the checklist. Sometimes it helps to read other people's stories. These case studies of domestic abuse highlight some real stories.
In today's webinar, we are focusing on a case study to help illustrate how women affected by domestic and family violence might experience our service systems. We'll reflect on this case study to look at how policies and practices can be improved helping sure women receive the support they need.
Section 2 provides a comprehensive review of the relevant literature on household violence. Section 3 presents the case study that forms the basis of this research. ... where religious texts such as the Bible and the Qur'an are often quoted to justify and perpetuate gender-based violence . For example, in the book of Ephesians 5:22-24, the ...
Violence against women is one of the most widespread, persistent and detrimental violations of human rights in today's world, which has not been reported in most cases due to impunity, silence, stigma and shame, even in the age of social communication. Domestic violence against women harms individuals, families, and society. The objective of this study was to investigate the prevalence and ...
Physical Abuse; Physical abuse may consist of various behaviors such as hitting, shoving, slapping, pinching, grabbing, biting, and hair pulling, among other physical abuse. In addition, the abuse may include denying individual medical attention or forcing drugs or alcohol upon a partner. Economic Abuse; Economic abuse involves controlling or ...
CASE 1. An 18-year-old woman presented to her family physician for an initial obstetric examination, accompanied by her 27-year-old boyfriend. Initial history revealed that she was a gravida 1 ...
Case study: Intimate partner violence [resident version] 1. Describe key assessment data to collect in suspected cases of intimate partner violence. 2. Determine the public health nurse's legal responsibility in reporting intimate partner violence. 3. Discuss the health determinants and factors that increase risk for intimate partner violence. 4.
Miremba and James were married in Uganda on June 10th, 2005. It was the first marriage for both. It was only after their marriage that Miremba discovered that James had a child from a previous relationship. James had a well-paying full-time job as a supervisor in a large grocery chain and he sponsored Miremba to immigrate to Canada.
Case Study/PSYS830 Aditya Putra Kurniawan/43160611 Case Study: Domestic Violence and Trauma Josie (25) is referred to you by her GP for depression. She lives with her husband (Greg, 27) and children (aged 2 and 4). She says she is not coping. She thinks she's going to get the sack from her part-time job because she's missed a few days ...
Swamy's abuse of Abi was a textbook case of "serious, high-risk domestic abuse", she says. There was coercive control and emotional abuse, isolation - Swamy discouraged her from seeing friends and ...
The research found that 21.3% of rural residents and 16.5% of urban residents who experienced intimate partner violence reported not receiving abuse screening. In addition, 40% of rural and 36.3% ...
Case Study: Intimate Partner Violence ... Sarah, for example, knows she shouldn't be 'letting' this happen to her, but is anxious about her ability to care for a new baby on her own, her financial well-being if she leaves, and her family's insistence that divorce is a sin. These may seem to be trivial, but for Sarah, these are her very ...