Academia.edu no longer supports Internet Explorer.
To browse Academia.edu and the wider internet faster and more securely, please take a few seconds to upgrade your browser .
Enter the email address you signed up with and we'll email you a reset link.
- We're Hiring!
- Help Center


Inclusive Education: Literature Review

The education of disabled children never received such amount of consideration and special efforts by government and non-government agencies in past as in present days. The attitude of the community in general and the attitude of parents in particular towards the education of the disabled have undergone change with the development of society and civilization.
Related Papers
vatika sibal
Executive Summary In India, inclusive education for children with disability has only recently been accepted in policy and in principle. In light of supportive policy and legislation, the present paper argues for individual initiative on part of an institution and colleges to implement programmes of inclusive education for children with disabilities in their classrooms. The paper provides guidelines in a generalized mode that institutions can follow to initiate such programmes. In this context, this paper argues for individual initiative on part of institutions to extend facilities for children with disabilities within their regular school settings. The paper further provides guidelines that institutions can adopt to set up inclusive education practices. The guidelines were derived from an empirical study which entailed examining prevalent practices and introducing inclusion in a regular institution setting. It is suggested that institutions can implement inclusive education programmes if they are adequately prepared, are able to garner support of all stakeholders involved in the process and have basic resources to run the programmes. The guidelines also suggest ways in which curriculum adaptations, teaching methodology and evaluation procedures can be adapted to suit needs of students with special needs. Issues of role allocation and seeking support of parents and peers are also dealt with. The recommendations that intuitions can adopt to implement inclusive education programmes for students with special needs within their regular set ups. The recommendations have been presented in a generalized mode to permit institute to interpret, modify and adapt the guidelines based on their individual needs and characteristics. It is pertinent those institutes that initiate such programmes assess their strengths and weaknesses at the outset and ensure adequate cooperation from the school management as well as the administrative and teaching staff. It is important to state here that an inclusive education programme does not require resource overload or elaborate preparations. With policy support, opportunities for training of teachers and cooperation from parents and the peer group, inclusive practices can be effectively adopted by any school. Clarity of vision, commitment to the goal of inclusion, and a perceptible understanding of the nuances involved in such an initiative are central to the success of the programme. Emotional commitment to inclusion emerges when the intellectual understanding of the concept goes through a democratic visioning process involving all the stakeholders expressing their opinions and feelings.
Inclusive Education: children with disabilities - - Background paper prepared for the 2020 Global Education Monitoring Report Inclusion and education 2020
Paula Frederica Hunt
This paper presents the case for inclusive education for children with disabilities as the entry point for policy development and implementation of inclusive education in the broad sense: inclusive, quality education for ALL children. The paper starts by providing a short historical perspective of the education of children with disabilities and continues with a description of the essential elements of an inclusive legislative framework, with a particular focus on General Comment no4 of Article 24 (CRPD). The benefits of inclusive education, as well as financing mechanisms, and required accountability measures for implementation, are also discussed. Then, the paper discusses the foundational basis of curriculum for inclusion, as well as issues related to a transformative teacher education practice. The final chapters describe what an inclusive school might look like, as well as the role of students, families and communities in creating an inclusive education system. It should be noted that this paper is substantiated with selective literature, with attention payed to an equitable geographic coverage.
ankur madan
Research Anthology on Inclusive Practices for Educators and Administrators in Special Education
Shekh Farid
BRAC, a leading international development organization, has been working to ensure the rights of persons with disabilities to education through its inclusive education program. This article discusses the BRAC approach in Bangladesh and aims to identify its strategies that are effective in facilitating inclusion. It employed a qualitative research approach where data were collected from students with disabilities, their parents, and BRAC's teachers and staffs using qualitative data collection techniques. The results show that the disability-inclusive policy and all other activities are strongly monitored by a separate unit under BRAC Education Program (BEP). It mainly focuses on sensitizing its teachers and staff to the issue through training, discussing the issue in all meetings and ensuring effective use of a working manual developed by the unit. Group-based learning and involving them in income generating activities were also effective. The findings of the study would be usefu...
Shonazar Botirov
This article describes the introduction of inclusive education, what it is, about children with disabilities, as well as the positive and negative aspects of inclusive education.
Ikhfi Imaniah
This paper identifies and discusses major issues and trends in special education in Indonesia, including implications of trends for the future developments. Trends are discussed for the following areas: (1) inclusion and integration, issues will remain unresolved in the near future; (2) early childhood and postsecondary education with disability students, special education will be viewed as lifespan schooling; (3) transitions and life skills, these will receive greater emphasis; and (4) consultation and collaboration, more emphasis but problems remain. Moreover, the participant of the study in this paper was an autism student of twelve years old who lived at Maguwoharjo, Yogyakarta. This study was qualitative with case study as an approach of the research. The researchers conclude the autism that has good academic, communication and emotional skill are able to go to integrated school accompanied by guidance teacher. But in practice, inclusive education in Indonesia is inseparable from stakeholders ranging from government and institutions such as schools, educators, school environment, community and parents to support the goal of inclusive education itself. Adequate infrastructure also needs to be given to the school that organizes inclusive education for an efficient and effective students understanding learning-oriented of inclusive education. In short, every child has the same opportunity in education, yet for special education which is aimed at student with special educational needs.
Rajendra KR
Inclusive Education on Children with Learning Disabilities
Arien Arien
ABSTRACT Name : Zahrien Assyifa Nur Palisma NISN : 0002223086 Title : Analysis of Inclusive Education on Children with Learning Disabilities (Case study on 4th Grade of Mutiara Bunda Elementary School, Cilegon Banten Inclusive Education is an approach that aims to change the education system by translating barriers that can accommodate every student to participate fully in education. That is, every child is entitled to a decent education, not to mention children with learning disabilities. Children with learning disabilities are interpreted as children who find it difficult to receive formal and non-formal learning because of certain psychological "disabilities". This study aims to determine how much the effectiveness of inclusive education for children with learning disabilities in Mutiara Bunda Elementary School, Cilegon. The method used by the author is the field research that is carried out on October 6th, 2017 at Bunda Mutiara Elementary School, Street. Boulevard Raya Block A2 Number.6 Taman Cilegon Indah, Sukmajaya, Cilegon Banten.The results obtained from this study are: a. Inclusive Education is the right solution for children with learning disabilities even for all children with disabilities. b. The curriculum used in inclusive schools is similar to the curriculum in public schools. There is little modification in children with learning disabilities as well as some omissions and curriculum substitutions. Keywords: Inclusive Education, Children with Learning Disabilities
Swati Chakraborty
International Journal of …
Missy Morton
RELATED PAPERS
American Yearbook of International Law – AYIL, Volume 2
Virginia Balafouta
História da Educação
Danilo Romeu Streck
Journal of Surgical Research
Indonesian Journal of Tropical and Infectious Disease
prihartini widiyanti
Ecological Applications
Joseph O'Brien
Marilda Martins Fayad
Engineering in Life Sciences
oluwaseun Adelaja
Jan Pralits
Howard Liddle
Journal of Oral Implantology
Sebastiano Andreana
Koko Warner
Enzyme and Microbial Technology
Dr Rooma Devi
Mats Wiklund
Procedia CIRP
Erik Sundin
Biochemical pharmacology
Education + Training
Bayan Ustwani
Türk Kütüphaneciliği
Mehmet Toplu
Zhenming Wang
hemangi bawane
Mathematics in industry
Rick Janssen
Radiotherapy and Oncology
Cristiana Fodor
RELATED TOPICS
- We're Hiring!
- Help Center
- Find new research papers in:
- Health Sciences
- Earth Sciences
- Cognitive Science
- Mathematics
- Computer Science
- Academia ©2024
Review of Literature: Inclusive Education
This brief review of relevant literature on inclusive education forms a component of the larger Inclusive School Communities Project: Final Evaluation Report delivered by the Research in Inclusive and Specialised Education (RISE) team to JFA Purple Orange in October, 2020.
Suggested citation for full evaluation report:
Jarvis, J. M., McMillan, J. M., Bissaker, K., Carson, K. L., Davidson, J., & Walker, P. M. (2020). Inclusive School Communities Project: Final Evaluation Report. Research in Inclusive and Specialised Education (RISE), Flinders University.
https://sites.flinders.edu.au/rise
Introduction
Inclusive education has featured prominently in worldwide educational discourse and reform efforts over the past 30 years (Berlach & Chambers, 2011; Forlin, 2006). Inclusive schools are critical to providing a strong foundation for young people with disabilities to access, participate in and contribute to their communities and lead fulfilling lives (Hehir et al., 2016). Schools also represent a key condition for the development of thriving, inclusive communities for all citizens. Yet, as reflected in submissions to the current Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability, and consistent with recent South Australian reports (Parliament of South Australia, 2017; Walker, 2017), many students living with disability (and their families) continue to report negative experiences of education. While progress has been made, traditional educational structures and practices often run counter to inclusive goals (Slee, 2013), and inconsistencies occur between theory and policy and the implementation of inclusive principles and practices in schools (Carrington & Elkins, 2002; Graham & Spandagou, 2011). In addition, both preservice and practicing teachers consistently report feeling underprepared to teach students with disabilities and special educational needs (Jarvis, 2019; OECD, 2019).
Despite legislation and policy imperatives related to inclusive education, there remains a lack of consensus in the field about the definition of inclusion and associated models of inclusive practice (Ainscow & Sandill, 2010; Kinsella, 2020). Multiple conceptualisations of inclusion and theoretical approaches to fostering inclusion in schools may contribute to confusion and uncertainty for educators and policymakers. With schools facing growing accountability and teachers expected to educate an increasingly diverse student population (Anderson & Boyle, 2015), it is vital that the concept of inclusive education is demystified for practitioners. Against this backdrop, initiatives such as the Inclusive School Communities (ISC) project that aim to deepen understandings of inclusion and increase the capacity of school communities to provide an inclusive education, are particularly important.
Inclusive Education
Inclusive education is based on a philosophy that stems from principles of social justice, and is primarily concerned with mitigating educational inequalities, exclusion, and discrimination (Anderson & Boyle, 2015; Booth, 2012; Waitoller & Artiles, 2013). Although inclusion was originally concerned with ‘disability’ and ‘special educational needs’ (Ainscow et al., 2006; Van Mieghem et al., 2020), the term has evolved to embody valuing diversity among all students, regardless of their circumstances (e.g., Carter & Abawi, 2018; Thomas, 2013). Among interpretations of inclusion, common themes include fairness, equality, respect, diversity, participation, community, leadership, commitment, shared vision, and collaboration (Booth, 2012; McMaster, 2015). The United Nations Convention on the Rights of Persons with Disabilities (CRPD), to which Australia is a signatory, defines inclusive education as:
. . . a process of systemic reform embodying changes and modifications in content, teaching methods, approaches, structures and strategies in education to overcome barriers with a vision serving to provide all students of the relevant age range with an equitable and participatory learning experience and environment that best corresponds to their requirements and preferences. (United Nations, 2016, para 11)
Consistent with this definition, inclusive education now generally refers to the process of addressing the learning needs of all students, through ensuring participation, achievement growth, and a sense of belonging, enabling all students to reach their full potential (Anderson & Boyle, 2015; Booth, 2012; Stegemann & Jaciw, 2018). Inclusion is concerned with identifying and removing potential barriers to presence (attendance, access), meaningful participation, growth from an individual starting point, and feelings of connectedness and belonging for all students and community members, with a focus on those at particular risk of marginalisation or exclusion (Ainscow et al., 2006; Forlin et al., 2013).
Critically, the view of inclusion described above moves beyond considerations of the physical placement of a student in a particular setting or grouping configuration. That is, while physical access to a mainstream school environment is essential to maintain the rights of students living with disabilities to access education “on the same basis” as their peers (consistent with legislation and human rights principles), it is not sufficient to ensure inclusion. Rather, inclusion can be considered a multi-faceted approach involving processes, practices, policies and cultures at all levels of a school and system (Booth & Ainscow, 2011). Inclusive education is responsive to each child and promotes flexibility, rather than expecting the child to change in order to ‘fit’ rigid schooling structures. The latter approach reflects integration, and inclusion is also inconsistent with segregation, in which children with disabilities are routinely educated separately from others.
Considerable research has focused on the implementation of inclusive school processes, practices and cultures that are sustainable over time. Although a number of frameworks to achieve sustainable inclusive practice have been proposed, key elements are consistent across approaches and well supported by research (Booth & Ainscow 2011; Azorín & Ainscow, 2020). These interconnected elements are summarised in Figure 1 and considered fundamental to the process of achieving whole-school (and systemic) cultural change towards more inclusive ways of working. Of particular relevance to the Inclusive School Communities project are the concepts of a whole school approach, leadership, school values and culture, building staff capacity, and multi-tiered models of inclusive practice.
Inclusion as a Whole School Approach
Adopting a whole of school approach to inclusive education is fundamental to ensure efficacy and sustainability (Read et al., 2015). The process of developing inclusive schools is complex and multi-faceted, requiring time, commitment, ongoing reflection, and sustained effort. For inclusion to truly take root in schools, changes must be made from the inside out; a strong foundation must be built from inclusive school values, committed leadership, and shared vision amongst staff to support whole school structural reforms to policy, pedagogy, and practice (Ekins & Grimes, 2009). Whilst challenging, “it is necessary to unsettle default modes of operation” in schools (Johnston & Hayes, 2007, p.376), as inclusive education requires new, more efficient and effective ways of supporting student participation and achievement. This is made possible by implementing flexible, planned whole school support structures, such as multi-tiered systems of support (MTSS), where teachers work collaboratively with specialist staff to identify, monitor, and support students requiring varying levels and types of intervention at different times, and for different purposes (Sailor, 2017; Witzel & Clarke, 2015). This contrasts to the more traditional, ‘categorical’ and segregated approach of general educators referring identified students with additional needs to special educators, to devise and administer further education in isolation from the regular classroom (Sailor, 2017).
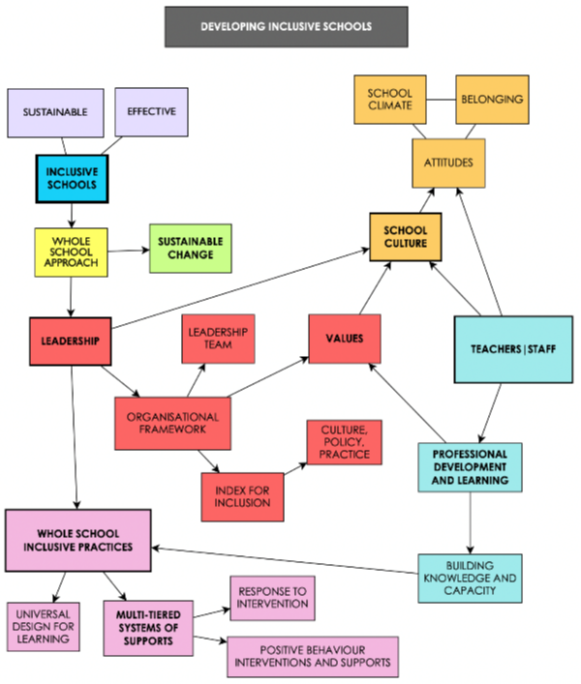
Figure 1. Interconnected elements in sustainable inclusive education, derived from research.
Even at the classroom level, inclusive planning and teaching practices must be supported by school policies, practices, and culture in order to be sustainable (Sailor, 2017). Barriers to inclusive classroom practice can include lack of effective professional learning and support for teachers; teachers’ lack of willingness to include students with particular needs; attitudes that are inconsistent with inclusive practices; teacher education that fails to address concerns about inclusion; and, a lack of accountability for the implementation of inclusive teaching practices (Forlin & Chambers, 2011; Forlin et al., 2008; van Kraayenoord et al., 2014). Addressing each of these relies on targeted, coordinated support. The complexity of embedding inclusive practices such as differentiated instruction or Universal Design for Learning (UDL) into classroom work is often underestimated, and these practices have the greatest chance of becoming embedded when they are reinforced by a shared vision and collaborative effort (McMaster, 2013; Sailor, 2015; Tomlinson & Murphy, 2017).
Sustainable, whole school change cannot be achieved via focus on a single element of inclusion in isolation, as components do not function in isolation. Rather, the core elements of inclusion including leadership, school culture, building staff capacity, and inclusive practices are parts of an interdependent system. Hence, key elements of inclusion must be considered collectively and accounted for in advanced planning to ensure they function harmoniously and are integrated into the developing inclusive fabric of the school (Alborno & Gaad, 2014).
Leadership for Inclusion
The importance of leadership for determining the success of school reforms or changes to practice is well established in the literature (McMaster & Elliot, 2014; Poon-McBrayer & Wong, 2013). Becoming a more inclusive school often requires significant shifts in school values, culture, practices, and organisational systems; thus, leadership is critical to ensuring sustainable inclusive change in schools (Ainscow & Sandill, 2010; McMaster, 2015; Poon-McBrayer & Wong, 2013). School leaders are highly influential figures whose values, beliefs, and actions directly affect the culture of the school, expectations of staff, and school operations (Slater, 2012; Wong & Cheung, 2009). It is critical that school leaders are committed to embodying inclusive principles, establishing and modelling a standard of behaviour that promotes the development of inclusion within the school community.
Organisational change on the scale often required for inclusion requires leadership across multiple levels (Jarvis et al., 2016; Tomlinson et al., 2008). It is likely to be most effective when facilitated through models of distributed leadership across roles and levels within a school, and when the case for change is underpinned by a broader, shared vision specifically related to student outcomes (Harris, 2013). Research has established the relationship between distributed leadership practices and the implementation of effective, inclusive school practices (Miškolci et al., 2016; Mullick et al., 2013; Robinson et al., 2008; Sharp et al., 2020). Leaders should consider utilising inclusive styles of management, replacing hierarchical structures with leadership teams (Ainscow & Sandill, 2010; McMaster, 2015). Effective school leadership enables shared responsibility, vision, and consistency within the school community, which is vital for the successful implementation of inclusion (Poon- McBrayer & Wong, 2013).
Fostering Inclusive School Cultures
Developing an inclusive school culture is a fundamental component of developing sustainable inclusion in schools (Dyson et al., 2004; McMaster, 2013). The culture of a school is made up of the shared values, attitudes, and beliefs of the school community (Booth, 2012). Transitioning to a truly inclusive culture requires close attention to attitudes and general support of the inclusive values being adopted, particularly by staff, but also by students and the broader school community (Dyson et al., 2004; Forlin & Chambers, 2011).
A whole school approach to inclusion prompts a school to reflect on and embrace values based on inclusive principles, such as equality, diversity, and respect. This process cannot be imposed, but should be a collaborative exercise with school leaders and staff, to ensure any pedagogical philosophies or practices based on outdated ideas or past assumptions are not operating by default (Johnston & Hayes, 2007; Schein, 2004). Evaluating and redefining existing school values also requires professional learning, to facilitate a collective reconceptualisation of inclusion specific to the unique context of the school; the meaning, aims, and expectations of inclusion must be clarified for the school community, to encourage a shared understanding, vision, and responsibility for supporting the inclusive changes unfolding within the school (Horrocks et al., 2008; Symes & Humphrey, 2011). Finally, it is vital that school policies and practices are regularly revised, to ensure that they reinforce the inclusive values and culture of the school; otherwise, they can act as a potential barrier to the development of sustainable whole school inclusion (Dybvik, 2004; McMaster, 2013).
Building Teachers’ Capacity for Inclusive Practice
Building the knowledge and capacity of teachers and other school staff is crucial to developing sustainable inclusion in schools. The evolution of an inclusive school culture depends on aligning the attitudes and behaviour of staff (McMaster, 2015). Teachers must be knowledgeable about how inclusive education has progressed over time, particularly how the meaning of inclusion has changed and what it means in their school context. Understanding the concepts and values behind inclusion can help teachers appreciate its significance, prompting reflection of their own practice and how they see their students (Anderson & Boyle, 2015; Skidmore, 2004). This can allow any unhelpful assumptions or beliefs that may have been unconsciously informing their teaching practice, particularly in relation to students living with disability, to be challenged and revised (Ashby, 2012; Ashton & Arlington, 2019).
While attention to attitudes, values, and broad understandings is fundamental, the goals of inclusion will only be achieved when principles are consistently enacted in daily classroom practice. At the classroom level, inclusion relies on teachers’ willingness and capacity to apply evidence-informed inclusive practices, such as Universal Design for Learning (UDL) and Differentiated Instruction (Van Mieghem et al., 2020). UDL is a planning framework for learning activities designed to maximise curriculum accessibility for all students by offering multiple opportunities for engagement, representation, and action and expression (CAST, 2018; Sailor, 2015). Differentiated Instruction (DI) is a holistic framework of interdependent principles and practices that enables teachers to design learning experiences to address variation in students’ readiness, interests and learning preferences (Tomlinson, 2014). UDL is primarily focused on inclusive task design, although the model has been expanded in recent years to include greater attention to pedagogy. Differentiation encompasses elements of planning (clear, concept-based learning objectives; formative assessment to inform proactive decision-making for diverse students), teaching (strategies to differentiate by readiness, interest and learning preference; ensuring respectful tasks and ‘teaching up’), and learning environment (flexible grouping, classroom management, establishing an inclusive culture) (Jarvis, 2015; Tomlinson, 2014).
The application of UDL and DI principles and practices by skilled teachers enables diverse students to access curriculum content in multiple ways (Kozik et al., 2009; McMaster, 2013), at appropriate levels of challenge and support to ensure learning growth, and in ways that support motivation, engagement, and feelings of connection and belonging (Beecher & Sweeney, 2008; Callahan et al., 2015; van Kraayenoord, 2007; Stegemann & Jaciw, 2018). These complementary frameworks apply to all students and define general, flexible classroom practices that also reduce the need for individualised adjustments for students with identified disabilities and specialised learning needs. However, in inclusive classrooms, teachers must also develop the knowledge and skills to make and implement reasonable adjustments and accommodations that enable students with identified disabilities and more complex needs to engage with curriculum and assessment ‘on the same basis’ as their peers, as defined within the Disability Standards for Education (Davies et al., 2016).
While inclusive teaching and classroom practices are non-negotiable, the challenge for some teachers to master the necessary skills and achieve the significant shift away from traditional teaching practices is often underestimated (Dixon et al., 2014; Tomlinson & Murphy, 2015). It is well-documented that teachers often find it difficult to apprehend both the conceptual and practical tools of DI and to embed differentiated practices into their daily work (Dack, 2019), particularly when they are not adequately resourced or supported to do so (Black-Hawkins & Florian, 2012; Brigandi et al., 2019; Fuchs et al., 2010; Mills et al, 2014). Perhaps related to teachers’ perceived lack of competence and confidence, the past 5-10 years have seen an enormous increase in the employment of teacher aides to work alongside students with disabilities in mainstream classrooms, despite limited evidence for its effectiveness and often in the context of inadequate planning and oversight (e.g., Sharma & Salend, 2016).
Engagement in targeted professional learning (PL) is fundamental to supporting the shift towards inclusive teaching. Yet, traditional approaches to PL have been criticised for a lack of systematic evaluation and inadequate adherence to principles of effectiveness (Avalos, 2011; Merchie et al., 2018). Research on effective professional learning for teachers has established common principles and practices that are associated with changes in practice, and these also align with teachers’ stated preferences (Walker et al., 2018). These include:
- professional learning is embedded in teachers’ own work contexts, and requires teachers to engage with content that is highly relevant to their daily practice, and closely linked to student learning (Desimone, 2009; Easton, 2008; Spencer, 2016; Van den Bergh et al., 2014);
- professional learning enables teachers to learn together with colleagues, such as in communities of practice (Gore et al., 2017; Voelkel & Chrispeels, 2017);
- professional learning activities are supported by robust school leadership and linked to broader school values and goals (Carpenter, 2015; Frankling et al., 2017; Sharp et al., 2020; Tomlinson et al., 2008; Whitworth & Chiu, 2015);
- professional learning is provided over extended periods, is led by facilitators with expert knowledge, and includes timely follow up activities such as mentoring and coaching to embed changes in practice (Desimone & Pak, 2017; Grierson & Woloshyn, 2013; Tomlinson & Murphy, 2015).
Multi-tiered Approaches to Whole School Inclusive Practice
Multi-tiered system of supports (MTSS) is an overarching term for a whole school inclusive framework that can be used to structure the flexible, timely distribution of resources to support students depending on their level of need (Sailor, 2017). As reflected in the generic depiction of MTSS in Figure 2, models generally utilise three tiers of intervention and teaching, where the intensity of the support is increased with each level or tier (McLeskey et al, 2014; Witzel & Clarke, 2015). Tier 1 includes core differentiated instruction and universal, evidence-based strategies for support that all students in the class receive. Tier 2 provides additional, targeted support to certain students for a specified purpose and period of time, usually in a small group format, while Tier 3 represents the most intensive and individualised support (Webster, 2016). The MTSS approach requires assessing all students regularly to assist in the early identification of needs requiring additional support, to enable prompt delivery of targeted interventions (McLeskey et al., 2014). MTSS is concerned with supporting the holistic development of students, by targeting their academic progress, behaviour, and socio-emotional well- being (McMillan & Jarvis, 2017).
When implemented with fidelity, MTSS is an effective whole school inclusive framework as teachers, therapists, and other support staff work collaboratively to assess, monitor, and plan interventions to support students (Sailor, 2017). Student progress is frequently monitored and data are evaluated by the support team to determine whether alternative interventions are required. MTSS additionally encourages the use of evidence-based practices to be implemented across the tiers of support. Some common examples of MTSS include Response to Intervention (RTI) and Positive Behaviour Interventions and Supports (PBIS) (Webster, 2016). RTI is focused on supporting students academically, while PBIS is concerned with emphasising behavioural expectations in a positive manner, naturally supporting the social and emotional development of students. MTSS models have also been applied in whole-school mental health promotion, prevention and intervention (McMillan & Jarvis, 2017) and inclusive approaches to academic talent development for more advanced students (Jarvis, 2017).
MTSS approaches to contemporary inclusive practice stand in contrast to traditional, categorical models whereby students were either ‘in’ or ‘out’ of special education services. The focus is on determining and responding to what students need when they need it, as opposed to focusing on a specific diagnosis or inflexible program options. In the MTSS framework, the tiers do not represent students or their placement, but the flexible suite of supports and interventions that may be provided. The implementation of MTSS approaches fundamentally reconceptualises the role of the classroom teacher, who must work collaboratively with specialist staff and other professionals to define and address individual student needs in ongoing ways, rather than relying on a specialist teacher or even a teacher aide to take responsibility for the education of students with identified special needs. While MTSS requires substantial changes to school operations (and must therefore be supported by leadership and culture in deliberate, coordinated ways), the general framework provides an organisation and structure to support the development of sustainable, contemporary inclusive schools (McLeskey et al., 2014).
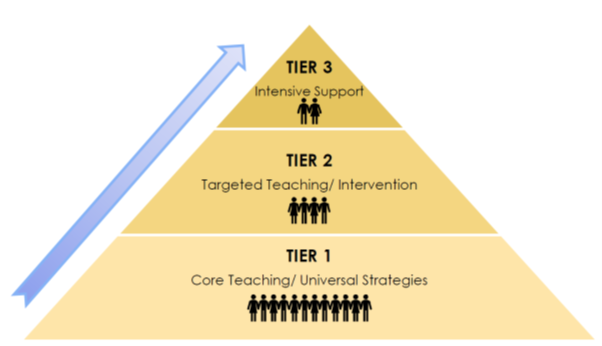
Figure 2. Multi-tiered System of Supports (MTSS) framework.
Conclusion
Ultimately, developing sustainable and effective inclusion in schools is a challenging but worthwhile undertaking, requiring shared vision, commitment, ongoing reflection, and patience. Changes in practice, particularly in teachers’ daily planning and pedagogy, take time and will be supported by ongoing, well designed and embedded professional learning in the context of strong leadership and an inclusive school culture. By utilising a whole school approach, key areas including leadership, school values and culture, building staff capacity, and coordinated frameworks for inclusive practice, can be considered collectively and planned for in advance.
References
Ainscow, M., & Sandill, A. (2010). Developing inclusive education systems: The role of organizational cultures and leadership. International Journal of Inclusive Education, 14 (4), 401–416. https://doi.org/10.1080/13603110802504903
Ainscow, M., Booth, T., & Dyson, A. (2006). Improving Schools, Developing Inclusion. Routledge.
Alborno, N., & Gaad, E. (2014). Index for Inclusion: A framework for school review in the United Arab Emirates. British Journal of Special Education, 41 (3), 231–248. https://doi.org/10.1111/1467-8578.12073
Anderson, J., & Boyle, C. (2015). Inclusive education in Australia: Rhetoric, reality and the road ahead. Support for Learning, 30 (1), 4–22. https://doi.org/10.1111/1467-9604.12074
Ashby, C. (2012). Disability studies and inclusive teacher preparation: A socially just path for teacher education. Research and Practice for Persons with Severe Disabilities, 37 (2), 89–99. https://doi.org/10.1177%2F154079691203700204
Ashton, J. R., & Arlington, H. (2019). My fears were irrational: Transforming conceptions of disability in teacher education through service learning. International Journal of Whole Schooling, 15 (1), 50–81.
Askell-Williams, H., & Koh, G. (2020). Enhancing the sustainability of school improvement initiatives. School Effectiveness and School Improvement. https://doi.org/10.1080/09243453.2020.1767657
Avalos, B. (2011). Teacher professional development in teaching and teacher education over ten years. Teaching and Teacher Education, 27, 10–20. https://doi.org/10.1016/j.tate.2010.08.007
Beecher, M., & Sweeney, S. M. (2008). Closing the achievement gap with curriculum enrichment and differentiation: One school’s story. Journal of Advanced Academics, 19 (3), 502–530. https://doi.org/10.4219/jaa-2008-815
Berlach, R. G., & Chambers, D. J. (2011). Interpreting inclusivity: An endeavour of great proportions. International Journal of Inclusive Education, 15, 529–539. https://doi.org/10.1080/13603110903159300
Black-Hawkins, K. & Florian, L. (2012). Classroom teachers’ craft knowledge of their inclusive practice. Teachers and Teaching: Theory and Practice, 8 (5), 567–584. https://doi.org/10.1080/13540602.2012.709732
Booth, T. (2012). Creating welcoming cultures: The index for inclusion. Race Equality Teaching, 30 (2), 19–21. http://doi.org/10.18546/RET.30.2.07
Booth, T., & Ainscow, M. (2011). Index for Inclusion: developing learning and participation in schools (3rd ed.). Centre for Studies on Inclusive Education. http://www.csie.org.uk/resources/inclusion-index-explained.shtml
Brigandi, C., Gibson, C. M., & Miller, M. (2019). Professional development and differentiated instruction in an elementary school pull-out program: A gifted education case study. Journal for the Education of the Gifted, 42 (4), 362–395. https://doi.org/10.1177/0162353219874418
Callahan, C. M., Moon, T. R., Oh, S., Azano, A. P., & Hailey, E. P. (2015). What works in gifted education: Documenting the effects of an integrated curricular/instructional model for gifted students. American Education Research Journal, 52, 137–167. https://doi.org/10.3102/0002831214549448
Carpenter, D. (2015). School culture and leadership of professional learning communities. International Journal of Educational Management, 29 (5), 682–694. https://doi.org/10.1108/IJEM-04-2014-0046
Carrington, S., & Elkins, J. (2002). Bridging the gap between inclusive policy and inclusive culture in secondary schools. Support for Learning, 17 (2), 51–57.
Carter, S., & Abawi, L. (2018). Leadership, inclusion, and quality education for all. Australasian Journal of Special and Inclusive Education, 42 (1), 49–64. https://doi.org/10.1017/jsi.2018.5
CAST. (2018). Universal Design for Learning Guidelines Version 2.2. http://udlguidelines.cast.org
Davies, M., Elliott, S., & Cumming, J. (2016). Documenting support needs and adjustment gaps for students with disabilities: Teacher practices in Australian classrooms and on national tests. International Journal of Inclusive Education, 20 (12), 1252–1269. https://doi.org/10.1080/13603116.2016.1159256
Desimone, L. M. (2009). Improving impact studies of teachers’ professional development: Toward better conceptualizations and measures. Educational Researcher, 38 (3),181–199. https://doi.org/10.3102/0013189X08331140
Desimone, L. M., & Pak, K. (2017). Instructional coaching as high-quality professional development. Theory Into Practice, 56 (1), 312. https://doi.org/10.1080/00405841.2016.1241947
Dixon, F. A., Yssel, N., McConnell, J. A., & Hardin, T. (2014). Differentiated instruction, professional development and teacher efficacy. Journal for the Education of the Gifted, 37 (2), 111–127. https://doi.org/10.1177/0162353214529042
Dybvik, A. C. (2004). Autism and the inclusion mandate: What happens when children with severe disabilities like autism are taught in regular classrooms? Daniel knows. Education Next, 4 (1), 42–49.
Dyson, A., Farrell, P., Polat, F., Hutcheson, G., & Gallanaugh, F. (2004). Inclusion and pupil achievement. Department for Education and Skills.
Easton, L. B. (2008). From professional development to professional learning. Phi Delta Kappan, 89, 755–761. https://doi.org/10.1177/003172170808901014
Ekins, A., & Grimes, P. (2009). Inclusion: Developing an Effective Whole School Approach. McGraw Hill Open University Press.
Forlin, C. (2006). Inclusive education in Australia ten years after Salamanca. European Journal of Psychology of Education, 21 (3), 265–277. https://doi.org/10.1007/BF03173415
Forlin, C., & Chambers, D. (2011). Teacher preparation for inclusive education: Increasing knowledge but raising concerns. Asia-Pacific Journal of Teacher Education, 39 (1), 17–32. https://doi.org/10.1080/1359866X.2010.540850
Forlin, C., Chambers, D. J., Loreman, T., Deppler, J., & Sharma, U. (2013). Inclusive education for students with disability: A review of the best evidence in relation to theory and practice. The Australian Research Alliance for Children and Youth. https://www.aracy.org.au/publicationsresources/command/download_file/id/246/filename/Inclusive_education_for_students_with_disability_-_A_review_of_the_best_evidence_in_relation_to_theory_and_practice.pdf73
Forlin, C., Keen, M., & Barrett. E. (2008). The concerns of mainstream teachers: Coping with inclusivity in an Australian context. International Journal of Disability, Development and Education, 55 (3), 251–264. https://doi.org/10.1080/10349120802268396
Frankling, T. W., Jarvis, J. M. & Bell. M. R. (2017). Leading secondary teachers’ understandings and practices of differentiation through professional learning. Leading and Managing, 23 (2), 72–86.
Fuchs, D., Fuchs, L. S., & Stecker, P. M. (2010). The ‘blurring’ of special education in a new continuum of general education placements and services. Exceptional Children, 76 (3), 301–323. https://doi.org/10.1177/001440291007600304
Gore, J., Lloyd, A., Smith, M., Bowe, J., Ellis, H., & Lubans, D. (2017). Effects of professional development on the quality of teaching: Results from a randomised controlled trial of Quality Teaching Rounds. Teaching and Teacher Education, 68, 91–113. https://doi.org/10.1016/j.tate.2017.08.007
Graham, L., & Spandagou, I. (2011). From vision to reality: Views of primary school principals on inclusive education in New South Wales, Australia. Disability & Society, 26 (2), 223–237. https://doi.org/10.1080/09687599.2011.544062
Grierson, A. L., & Woloshyn, V. E. (2013). Walking the talk: Supporting teachers’ growth with differentiated professional learning. Professional Development in Education, 39 (3), 401–419. https://doi.org/10.1080/19415257.2012.763143
Guskey, T. R. (2000). Evaluating professional development. Corwin Press
Harris, A. (2013). Distributed leadership: Friend or foe? Educational Management, Administration & Leadership, 4 (5), 545–554. https://doi.org/10.1177/1741143213497635
Hehir, T., Pascucci, S., & Pascucci, C. (2016). A summary of the evidence on inclusive education, Instituto Alana, 2. https://files.eric.ed.gov/fulltext/ED596134.pdf
Horrocks, J. L., White, G., & Roberts, L. (2008). Principals' attitudes regarding inclusion of children with autism in Pennsylvania public schools. Journal of Autism and Developmental Disorders, 38, 1462–1473. https://doi.org/10.1007/s10803-007-0522-x
Jarvis, J. M. (2015). Inclusive Classrooms and Differentiation. In N. Weatherby-Fell (Ed.), Learning to Teach in the Secondary School (pp. 154–171). Cambridge University Press.
Jarvis, J. M. (2019). Most Australian teachers feel unprepared to teach students with special needs. The Conversation. https://theconversation.com/most-australian-teachers-feel-unpreparedto-teach-students-with-special-needs-119227
Jarvis, J. M., (2017). Supporting diverse gifted students. In M. Hyde, L. Carpenter & S. Dole (Eds.), Diversity, Inclusion and Engagement (3rd ed., pp. 308–329). Oxford University Press.
Johnston, K., & Hayes, D. (2007). Supporting students’ success at school through teacher professional learning: The pedagogy of disrupting the default modes of schooling. International Journal of Inclusive Education, 11 (3), 371–381. https://doi.org/10.1080/13603110701240666
Kinsella, W. (2020). Organising inclusive schools. International Journal of Inclusive Education, 24 (12), 1340–1356. https://doi.org/10.1080/13603116.2018.1516820
Kozik, P., Cooney, B., Vinciguerra, S., Gradel, K., & Black, J. (2009). Promoting inclusion in secondary schools through appreciative inquiry. American Secondary Education, 38 (1), 77–91.
McLeskey, J., Waldron, N. L., Spooner, F., & Algozzine, B. (Eds.). (2014). Handbook of effective inclusive schools: Research and practice. Taylor & Francis.
McMaster, C. (2013). Building inclusion from the ground up: A review of whole school re-culturing programmes for sustaining inclusive change. International Journal of Whole Schooling, 9 (2), 1–24.
McMaster, C. (2015). Inclusion in New Zealand: The potential and possibilities of sustainable inclusive change through utilising a framework for whole school development. New Zealand Journal of Educational Studies, 50 (2), 239–253.
McMaster, C., & Elliot, W. (2014). Leading inclusive change with the Index for Inclusion: Using a framework to manage sustainable professional development. Journal of Educational Leadership, Policy and Practice, 29 (1), 82–93. https://doi.org/10.1007/s40841-015-0010-3
McMillan, J., & Jarvis, J. M. (2017). Supporting mental health and well-being: Promotion, prevention and intervention. In M. Hyde, L. Carpenter & S. Dole (Eds.), Diversity, inclusion and engagement (3rd ed., pp. 65–392). Oxford University Press.
Merchie, E., Tuytens, M., Devos, G., & Vanderlinde, R. (2018). Evaluating teachers’ professional development initiatives: Towards an extended evaluative framework. Research Papers in Education, 33 (2), 143–168. https://doi.org/10.1080/02671522.2016.1271003
Mills, M., Monk, S., Keddie, A., Renshaw, P., Christie, P., Geelan, D. & C. Gowlett, C. (2014). Differentiated learning: From policy to classroom. Oxford Review of Education, 40 (3), 331–348. https://doi.org/10.1080/03054985.2014.911725
Miškolci, J., Armstrong, D., & Spandagou, I. (2016). Teachers' perceptions of the relationship between inclusive education and distributed leadership in two primary schools in Slovakia and New South Wales (Australia). Journal of Teacher Education for Sustainability, 18 (2), 53–65. https://doi.org/10.1515/jtes-2016-001
Mullick, J., Sharma, U., & Deppeler, J. (2013). School teachers' perception about distributed leadership practices for inclusive education in primary schools in Bangladesh. School Leadership & Management, 33 (2), 151–168. https://doi.org/10.1080/13632434.2012.723615
OECD (2019). TALIS 2018 Results (Volume I): Teachers and School Leaders as Lifelong Learners. OECD Publishing. https://doi.org/10.1787/1d0bc92a-en.
Parliament of South Australia. (2017). Report of the select committee on access to the South Australian Education System for students with a disability. https://apo.org.au/sites/default/files/resource-files/2017-05/apo-nid94396.pdf
Poon-McBrayer, K., & Wong, P. (2013). Inclusive education services for children and youth with disabilities: Values, roles and challenges of school leaders. Children and Youth Services Review, 35 (9), 1520–1525. https://doi.org/10.1016/j.childyouth.2013.06.009
Read, K., Aldridge, J., Ala’i, K., Fraser, B., & Fozdar, F. (2015). Creating a climate in which students can flourish: A whole school intercultural approach. International Journal of Whole Schooling, 11 (2), 29–44. https://doi.org/1710-2146
Robinson, V. M. J., Lloyd, C. A., & Rowe, K. J. (2008). The impact of leadership on student outcomes: An analysis of the differential effects of leadership types. Educational Administration Quarterly, 44 (5), 635–674. https://doi.org/10.1177/0013161X08321509
Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability. (2019). Issues Paper: Education and Learning. https://disability.royalcommission.gov.au/system/files/2020-07/Issues-paper-Education-Learning.pdf
Sailor, W. (2015). Advances in schoolwide inclusive school reform. Remedial and Special Education, 36, 94–99. https://doi.org/10.1177/0741932514555021
Sailor, W. (2017). Equity as a basis for inclusive educational systems change. The Australasian Journal of Special Education, 41 (1), 1–17. https://doi.org/10.1017/jse.2016.12
Schein, E. (2004). Organizational culture and leadership (3rd ed.). Jossey-Bass.
Sharma, U., & Salend, S. (2016). Teaching assistants in inclusive classrooms: A systematic analysis of the international research. Australian Journal of Teacher Education, 41 (8), 118–134.
Sharp, K., Jarvis, J. M., & McMillan, J. M. (2020). Leadership for differentiated instruction: Teachers' engagement with on-site professional learning at an Australian secondary school. International Journal of Inclusive Education, 24 (8), 901–920. https://doi.org/10.1080/13603116.2018.1492639
Skidmore, D. (2004). Inclusion: The dynamic of school development. McGraw-Hill Education.
Slater, C. L. (2012). Understanding principal leadership: An international perspective and a narrative approach. Educational Management Administration & Leadership, 39 (2), 219–227. https://doi.org/10.1177/1741143210390061
Slee, R. (2013). How do we make inclusive education happen when exclusion is a political predisposition? International Journal of Inclusive Education: Making Inclusive Education Happen: Ideas for Sustainable Change, 17 (8), 895–907. https://doi.org/10.1080/13603116.2011.602534
Spencer, E. J. (2016). Professional learning communities: Keeping the focus on instructional practice. Kappa Delta Pi Record, 52 (2), 83–85. https://doi.org/10.1080/00228958.2016.1156544
Stegemann, K., & Jaciw, A. (2018). Making it logical: Implementation of inclusive education using a logic model framework. Learning Disabilities: A Contemporary Journal, 16 (1), 3–18.
Symes, W., & Humphrey, N. (2011). School factors that facilitate or hinder the ability of teaching assistants to effectively support pupils with autism spectrum disorders (ASD) in mainstream secondary schools. Journal of Research in Special Educational Needs, 11 (3), 153–161. https://doi.org/10.1111/j.1471-3802.2011.01196.x
Thomas, G. (2013). A review of thinking and research about inclusive education policy, with suggestions for a new kind of inclusive thinking. British Educational Research Journal, 39 (3), 473–490. https://doi.org/10.1080/01411926.2011.652070
Tomlinson, C. A. (2014). The differentiated classroom: Responding to the needs of all learners (2nd ed.). Association for Supervision and Curriculum Development.
Tomlinson, C. A., & Murphy, M. (2015). Leading for differentiation: Growing teachers who grow kids. Association for Supervision and Curriculum Development.
Tomlinson, C.A., Brimijoin, K., & Narvaez, L. (2008). The differentiated school: Making revolutionary changes in teaching and learning. Association for Supervision and Curriculum Development.
Van Den Bergh, L., Ros, A., & Beijaard, D. (2014). Improving teacher feedback during active learning: Effects of a professional development program. American Educational Research Journal, 51 (4), 772–809. https://doi.org/10.3102/0002831214531322
van Kraayenoord, C. E. (2007). School and classroom practices in inclusive education in Australia. Childhood Education, 83 (6), 390–394, https://doi.org/10.1080/00094056.2007.10522957
van Kraayenoord, C. E., Waterworth, D., & Brady. T. (2014). Responding to individual differences in inclusive classrooms in Australia. Journal of International Special Needs Education, 17 (2), 48–59.
Van Mieghem, A., Verschueren, K., Petry, K., & Struyf, E. (2020). An analysis of research on inclusive education: A systematic search and meta review. International Journal of Inclusive Education, 26 (6), 675–689. https://doi.org/10.1080/13603116.2018.1482012
Voelkel, R. H., Jr., & Chrispeels, J. H. (2017). Understanding the link between professional learning communities and teacher collective efficacy. School Effectiveness and School Improvement, 28, 505–526. https://doi.org/10.1080/09243453.2017.1299015
Waitoller, F. R., & Artiles, A. J. (2013). A decade of professional development research for inclusive education: A critical review and notes for a research program. Review of Educational Research, 83 (3), 319–356. https://doi.org/10.3102/0034654313483905
Walker, P. M., Carson, K. L., Jarvis, J. M., McMillan, J. M., Noble, A. G., Armstrong, D., . . . Palmer, C. (2018). How do educators of students with disabilities in specialist settings understand and apply the Australian Curriculum framework? Australasian Journal of Special and Inclusive Education, 42 (2), 111–126. https://doi.org/10.1017/jsi.2018.13
Webster, A. (2016). Utilising a leadership blueprint to build the capacity of schools to achieve outcomes for students with autism spectrum disorder. In G. Johnson & N. Dempster (Eds.), Leadership in diverse learning contexts (pp. 109–127). https://doi.org/10.1007/978-3-319-28302-9_6
Whitworth, B. A., & Chiu, J. L. (2015). Professional development and teacher change: The missing leadership link. Journal of Science Teacher Education, 26 (2), 121–137. https://doi.org/10.1007/s10972-014-9411-2
Inclusive School Communities Project Phone: (08) 8373 8333 Email: [email protected] Address: 104 Greenhill Road, Unley SA 5061
- Open access
- Published: 14 May 2024
Protocol for a scoping review study on learning plan use in undergraduate medical education
- Anna Romanova ORCID: orcid.org/0000-0003-1118-1604 1 ,
- Claire Touchie 1 ,
- Sydney Ruller 2 ,
- Victoria Cole 3 &
- Susan Humphrey-Murto 4
Systematic Reviews volume 13 , Article number: 131 ( 2024 ) Cite this article
Metrics details
The current paradigm of competency-based medical education and learner-centredness requires learners to take an active role in their training. However, deliberate and planned continual assessment and performance improvement is hindered by the fragmented nature of many medical training programs. Attempts to bridge this continuity gap between supervision and feedback through learner handover have been controversial. Learning plans are an alternate educational tool that helps trainees identify their learning needs and facilitate longitudinal assessment by providing supervisors with a roadmap of their goals. Informed by self-regulated learning theory, learning plans may be the answer to track trainees’ progress along their learning trajectory. The purpose of this study is to summarise the literature regarding learning plan use specifically in undergraduate medical education and explore the student’s role in all stages of learning plan development and implementation.
Following Arksey and O’Malley’s framework, a scoping review will be conducted to explore the use of learning plans in undergraduate medical education. Literature searches will be conducted using multiple databases by a librarian with expertise in scoping reviews. Through an iterative process, inclusion and exclusion criteria will be developed and a data extraction form refined. Data will be analysed using quantitative and qualitative content analyses.
By summarising the literature on learning plan use in undergraduate medical education, this study aims to better understand how to support self-regulated learning in undergraduate medical education. The results from this project will inform future scholarly work in competency-based medical education at the undergraduate level and have implications for improving feedback and supporting learners at all levels of competence.
Scoping review registration:
Open Science Framework osf.io/wvzbx.
Peer Review reports
Competency-based medical education (CBME) has transformed the approach to medical education to focus on demonstration of acquired competencies rather than time-based completion of rotations [ 1 ]. As a result, undergraduate and graduate medical training programs worldwide have adopted outcomes-based assessments in the form of entrustable professional activities (EPAs) comprised of competencies to be met [ 2 ]. These assessments are completed longitudinally by multiple different evaluators to generate an overall impression of a learner’s competency.
In CBME, trainees will progress along their learning trajectory at individual speeds and some may excel while others struggle to achieve the required knowledge, skills or attitudes. Therefore, deliberate and planned continual assessment and performance improvement is required. However, due to the fragmented nature of many medical training programs where learners rotate through different rotations and work with many supervisors, longitudinal observation is similarly fragmented. This makes it difficult to determine where trainees are on their learning trajectories and can affect the quality of feedback provided to them, which is a known major influencer of academic achievement [ 3 ]. As a result, struggling learners may not be identified until late in their training and the growth of high-performing learners may be stifled [ 4 , 5 , 6 ].
Bridging this continuity gap between supervision and feedback through some form of learner handover or forward feeding has been debated since the 1970s and continues to this day [ 5 , 7 , 8 , 9 , 10 , 11 ]. The goal of learner handover is to improve trainee assessment and feedback by sharing their performance and learning needs between supervisors or across rotations. However, several concerns have been raised about this approach including that it could inappropriately bias subsequent assessments of the learner’s abilities [ 9 , 11 , 12 ]. A different approach to keeping track of trainees’ learning goals and progress along their learning trajectories is required. Learning plans (LPs) informed by self-regulated learning (SRL) theory may be the answer.
SRL has been defined as a cyclical process where learners actively control their thoughts, actions and motivation to achieve their goals [ 13 ]. Several models of SRL exist but all entail that the trainee is responsible for setting, planning, executing, monitoring and reflecting on their learning goals [ 13 ]. According to Zimmerman’s SRL model, this process occurs in three stages: forethought phase before an activity, performance phase during an activity and self-reflection phase after an activity [ 13 ]. Since each trainee leads their own learning process and has an individual trajectory towards competence, this theory relates well to the CBME paradigm which is grounded in learner-centredness [ 1 ]. However, we know that medical students and residents have difficulty identifying their own learning goals and therefore need guidance to effectively partake in SRL [ 14 , 15 , 16 , 17 ]. Motivation has also emerged as a key component of SRL, and numerous studies have explored factors that influence student engagement in learning [ 18 , 19 ]. In addition to meeting their basic psychological needs of autonomy, relatedness and competence, perceived learning relevance through meaningful learning activities has been shown to increase trainee engagement in their learning [ 19 ].
LPs are a well-known tool across many educational fields including CBME that can provide trainees with meaningful learning activities since they help them direct their own learning goals in a guided fashion [ 20 ]. Also known as personal learning plans, learning contracts, personal action plans, personal development plans, and learning goals, LPs are documents that outline the learner’s roadmap to achieve their learning goals. They require the learner to self-identify what they need to learn and why, how they are going to do it, how they will know when they are finished, define the timeframe for goal achievement and assess the impact of their learning [ 20 ]. In so doing, LPs give more autonomy to the learner and facilitate objective and targeted feedback from supervisors. This approach has been described as “most congruent with the assumptions we make about adults as learners” [ 21 ].
LP use has been explored across various clinical settings and at all levels of medical education; however, most of the experience lies in postgraduate medical education [ 22 ]. Medical students are a unique learner population with learning needs that appear to be very well suited for using LPs for two main reasons. First, their education is often divided between classroom and clinical settings. During clinical training, students need to be more independent in setting learning goals to meet desired competencies as their education is no longer outlined for them in a detailed fashion by the medical school curriculum [ 23 ]. SRL in the workplace is also different than in the classroom due to additional complexities of clinical care that can impact students’ ability to self-regulate their learning [ 24 ]. Second, although most medical trainees have difficulty with goal setting, medical students in particular need more guidance compared to residents due to their relative lack of experience upon which they can build within the SRL framework [ 25 ]. LPs can therefore provide much-needed structure to their learning but should be guided by an experienced tutor to be effective [ 15 , 24 ].
LPs fit well within the learner-centred educational framework of CBME by helping trainees identify their learning needs and facilitating longitudinal assessment by providing supervisors with a roadmap of their goals. In so doing, they can address current issues with learner handover and identification as well as remediation of struggling learners. Moreover, they have the potential to help trainees develop lifelong skills with respect to continuing professional development after graduation which is required by many medical licensing bodies.
An initial search of the JBI Database, Cochrane Database, MEDLINE (PubMed) and Google Scholar conducted in July–August 2022 revealed a paucity of research on LP use in undergraduate medical education (UGME). A related systematic review by van Houten–Schat et al. [ 24 ] on SRL in the clinical setting identified three interventions used by medical students and residents in SRL—coaching, LPs and supportive tools. However, only a couple of the included studies looked specifically at medical students’ use of LPs, so this remains an area in need of more exploration. A scoping review would provide an excellent starting point to map the body of literature on this topic.
The objective of this scoping review will therefore be to explore LP use in UGME. In doing so, it will address a gap in knowledge and help determine additional areas for research.
This study will follow Arksey and O’Malley’s [ 26 ] five-step framework for scoping review methodology. It will not include the optional sixth step which entails stakeholder consultation as relevant stakeholders will be intentionally included in the research team (a member of UGME leadership, a medical student and a first-year resident).
Step 1—Identifying the research question
The overarching purpose of this study is to “explore the use of LPs in UGME”. More specifically we seek to achieve the following:
Summarise the literature regarding the use of LPs in UGME (including context, students targeted, frameworks used)
Explore the role of the student in all stages of the LP development and implementation
Determine existing research gaps
Step 2—Identifying relevant studies
An experienced health sciences librarian (VC) will conduct all searches and develop the initial search strategy. The preliminary search strategy is shown in Appendix A (see Additional file 2). Articles will be included if they meet the following criteria [ 27 ]:
Participants
Medical students enrolled at a medical school at the undergraduate level.
Any use of LPs by medical students. LPs are defined as a document, usually presented in a table format, that outlines the learner’s roadmap to achieve their learning goals [ 20 ].
Any stage of UGME in any geographic setting.
Types of evidence sources
We will search existing published and unpublished (grey) literature. This may include research studies, reviews, or expert opinion pieces.
Search strategy
With the assistance of an experienced librarian (VC), a pilot search will be conducted to inform the final search strategy. A search will be conducted in the following electronic databases: MEDLINE, Embase, Education Source, APA PsycInfo and Web of Science. The search terms will be developed in consultation with the research team and librarian. The search strategy will proceed according to the JBI Manual for Evidence Synthesis three-step search strategy for reviews [ 27 ]. First, we will conduct a limited search in two appropriate online databases and analyse text words from the title, abstracts and index terms of relevant papers. Next, we will conduct a second search using all identified key words in all databases. Third, we will review reference lists of all included studies to identify further relevant studies to include in the review. We will also contact the authors of relevant papers for further information if required. This will be an iterative process as the research team becomes more familiar with the literature and will be guided by the librarian. Any modifications to the search strategy as it evolves will be described in the scoping review report. As a measure of rigour, the search strategy will be peer-reviewed by another librarian using the PRESS checklist [ 28 ]. No language or date limits will be applied.
Step 3—Study selection
The screening process will consist of a two-step approach: screening titles/abstracts and, if they meet inclusion criteria, this will be followed by a full-text review. All screening will be done by two members of the research team and any disagreements will be resolved by an independent third member of the team. Based on preliminary inclusion criteria, the whole research team will first pilot the screening process by reviewing a random sample of 25 titles/abstracts. The search strategy, eligibility criteria and study objectives will be refined in an iterative process. We anticipate several meetings as the topic is not well described in the literature. A flowchart of the review process will be generated. Any modifications to the study selection process will be described in the scoping review report. The papers will be excluded if a full text is not available. The search results will be managed using Covidence software.
Step 4—Charting the data
A preliminary data extraction tool is shown in Appendix B (see Additional file 3 ). Data will be extracted into Excel and will include demographic information and specific details about the population, concept, context, study methods and outcomes as they relate to the scoping review objectives. The whole research team will pilot the data extraction tool on ten articles selected for full-text review. Through an iterative process, the final data extraction form will be refined. Subsequently, two members of the team will independently extract data from all articles included for full-text review using this tool. Charting disagreements will be resolved by the principal and senior investigators. Google Translate will be used for any included articles that are not in the English language.
Step 5—Collating, summarising and reporting the results
Quantitative and qualitative analyses will be used to summarise the results. Quantitative analysis will capture descriptive statistics with details about the population, concept, context, study methods and outcomes being examined in this scoping review. Qualitative content analysis will enable interpretation of text data through the systematic classification process of coding and identifying themes and patterns [ 29 ]. Several team meetings will be held to review potential themes to ensure an accurate representation of the data. The PRISMA Extension for Scoping Reviews (PRISMA-ScR) will be used to guide the reporting of review findings [ 30 ]. Data will be presented in tables and/or diagrams as applicable. A descriptive summary will explain the presented results and how they relate to the scoping review objectives.
By summarising the literature on LP use in UGME, this study will contribute to a better understanding of how to support SRL amongst medical students. The results from this project will also inform future scholarly work in CBME at the undergraduate level and have implications for improving feedback as well as supporting learners at all levels of competence. In doing so, this study may have practical applications by informing learning plan incorporation into CBME-based curricula.
We do not anticipate any practical or operational issues at this time. We assembled a team with the necessary expertise and tools to complete this project.
Availability of data and materials
All data generated or analysed during this study will be included in the published scoping review article.
Abbreviations
- Competency-based medical education
Entrustable professional activity
- Learning plan
- Self-regulated learning
- Undergraduate medical education
Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32(8):638–45.
Article PubMed Google Scholar
Shorey S, Lau TC, Lau ST, Ang E. Entrustable professional activities in health care education: a scoping review. Med Educ. 2019;53(8):766–77.
Hattie J, Timperley H. The power of feedback. Rev Educ Res. 2007;77(1):81–112.
Article Google Scholar
Dudek NL, Marks MB, Regehr G. Failure to fail: the perspectives of clinical supervisors. Acad Med. 2005;80(10 Suppl):S84–7.
Warm EJ, Englander R, Pereira A, Barach P. Improving learner handovers in medical education. Acad Med. 2017;92(7):927–31.
Spooner M, Duane C, Uygur J, et al. Self-regulatory learning theory as a lens on how undergraduate and postgraduate learners respond to feedback: a BEME scoping review : BEME Guide No. 66. Med Teach. 2022;44(1):3–18.
Frellsen SL, Baker EA, Papp KK, Durning SJ. Medical school policies regarding struggling medical students during the internal medicine clerkships: results of a National Survey. Acad Med. 2008;83(9):876–81.
Humphrey-Murto S, LeBlanc A, Touchie C, et al. The influence of prior performance information on ratings of current performance and implications for learner handover: a scoping review. Acad Med. 2019;94(7):1050–7.
Morgan HK, Mejicano GC, Skochelak S, et al. A responsible educational handover: improving communication to improve learning. Acad Med. 2020;95(2):194–9.
Dory V, Danoff D, Plotnick LH, et al. Does educational handover influence subsequent assessment? Acad Med. 2021;96(1):118–25.
Humphrey-Murto S, Lingard L, Varpio L, et al. Learner handover: who is it really for? Acad Med. 2021;96(4):592–8.
Shaw T, Wood TJ, Touchie T, Pugh D, Humphrey-Murto S. How biased are you? The effect of prior performance information on attending physician ratings and implications for learner handover. Adv Health Sci Educ Theory Pract. 2021;26(1):199–214.
Artino AR, Brydges R, Gruppen LD. Chapter 14: Self-regulated learning in health professional education: theoretical perspectives and research methods. In: Cleland J, Duning SJ, editors. Researching Medical Education. 1st ed. John Wiley & Sons; 2015. p. 155–66.
Chapter Google Scholar
Cleland J, Arnold R, Chesser A. Failing finals is often a surprise for the student but not the teacher: identifying difficulties and supporting students with academic difficulties. Med Teach. 2005;27(6):504–8.
Reed S, Lockspeiser TM, Burke A, et al. Practical suggestions for the creation and use of meaningful learning goals in graduate medical education. Acad Pediatr. 2016;16(1):20–4.
Wolff M, Stojan J, Cranford J, et al. The impact of informed self-assessment on the development of medical students’ learning goals. Med Teach. 2018;40(3):296–301.
Sawatsky AP, Halvorsen AJ, Daniels PR, et al. Characteristics and quality of rotation-specific resident learning goals: a prospective study. Med Educ Online. 2020;25(1):1714198.
Article PubMed PubMed Central Google Scholar
Pintrich PR. Chapter 14: The role of goal orientation in self-regulated learning. In: Boekaerts M, Pintrich PR, Zeidner M, editors. Handbook of self-regulation. 1st ed. Academic Press; 2000. p. 451–502.
Kassab SE, El-Sayed W, Hamdy H. Student engagement in undergraduate medical education: a scoping review. Med Educ. 2022;56(7):703–15.
Challis M. AMEE medical education guide No. 19: Personal learning plans. Med Teach. 2000;22(3):225–36.
Knowles MS. Using learning contracts. 1 st ed. San Francisco: Jossey Bass; 1986.
Parsell G, Bligh J. Contract learning, clinical learning and clinicians. Postgrad Med J. 1996;72(847):284–9.
Article CAS PubMed PubMed Central Google Scholar
Teunissen PW, Scheele F, Scherpbier AJJA, et al. How residents learn: qualitative evidence for the pivotal role of clinical activities. Med Educ. 2007;41(8):763–70.
Article CAS PubMed Google Scholar
van Houten-Schat MA, Berkhout JJ, van Dijk N, Endedijk MD, Jaarsma ADC, Diemers AD. Self-regulated learning in the clinical context: a systematic review. Med Educ. 2018;52(10):1008–15.
Taylor DCM, Hamdy H. Adult learning theories: Implications for learning and teaching in medical education: AMEE Guide No. 83. Med Teach. 2013;35(11):e1561–72.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalol H. Chapter 11: Scoping reviews. In: Aromataris E, Munn Z, eds. JBI Manual for Evidence Synthesis. JBI; 2020. https://synthesismanual.jbi.global. . Accessed 30 Aug 2022.
McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40–6.
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88.
Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73.
Venables M, Larocque A, Sikora L, Archibald D, Grudniewicz A. Understanding indigenous health education and exploring indigenous anti-racism approaches in undergraduate medical education: a scoping review protocol. OSF; 2022. https://osf.io/umwgr/ . Accessed 26 Oct 2022.
Download references
Acknowledgements
Not applicable.
This study will be supported through grants from the Department of Medicine at the Ottawa Hospital and the University of Ottawa. The funding bodies had no role in the study design and will not have any role in the collection, analysis and interpretation of data or writing of the manuscript.
Author information
Authors and affiliations.
The Ottawa Hospital – General Campus, 501 Smyth Rd, PO Box 209, Ottawa, ON, K1H 8L6, Canada
Anna Romanova & Claire Touchie
The Ottawa Hospital Research Institute, Ottawa, Canada
Sydney Ruller
The University of Ottawa, Ottawa, Canada
Victoria Cole
The Ottawa Hospital – Riverside Campus, Ottawa, Canada
Susan Humphrey-Murto
You can also search for this author in PubMed Google Scholar
Contributions
AR designed and drafted the protocol. CT and SH contributed to the refinement of the research question, study methods and editing of the manuscript. VC designed the initial search strategy. All authors reviewed the manuscript for final approval. The review guarantors are CT and SH. The corresponding author is AR.
Authors’ information
AR is a clinician teacher and Assistant Professor with the Division of General Internal Medicine at the University of Ottawa. She is also the Associate Director for the internal medicine clerkship rotation at the General campus of the Ottawa Hospital.
CT is a Professor of Medicine with the Divisions of General Internal Medicine and Infectious Diseases at the University of Ottawa. She is also a member of the UGME Competence Committee at the University of Ottawa and an advisor for the development of a new school of medicine at Toronto Metropolitan University.
SH is an Associate Professor with the Department of Medicine at the University of Ottawa and holds a Tier 2 Research Chair in Medical Education. She is also the Interim Director for the Research Support Unit within the Department of Innovation in Medical Education at the University of Ottawa.
CT and SH have extensive experience with medical education research and have numerous publications in this field.
SR is a Research Assistant with the Division of General Internal Medicine at the Ottawa Hospital Research Institute.
VC is a Health Sciences Research Librarian at the University of Ottawa.
SR and VC have extensive experience in systematic and scoping reviews.
Corresponding author
Correspondence to Anna Romanova .
Ethics declarations
Ethics approval and consent to participate, consent for publication, competing interests.
The authors declare that they have no competing interests.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. prisma-p 2015 checklist., 13643_2024_2553_moesm2_esm.docx.
Additional file 2: Appendix A. Preliminary search strategy [ 31 ].
Additional file 3: Appendix B. Preliminary data extraction tool.
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Romanova, A., Touchie, C., Ruller, S. et al. Protocol for a scoping review study on learning plan use in undergraduate medical education. Syst Rev 13 , 131 (2024). https://doi.org/10.1186/s13643-024-02553-w
Download citation
Received : 29 November 2022
Accepted : 03 May 2024
Published : 14 May 2024
DOI : https://doi.org/10.1186/s13643-024-02553-w
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Systematic Reviews
ISSN: 2046-4053
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]
- Open access
- Published: 14 May 2024
Developing a survey to measure nursing students’ knowledge, attitudes and beliefs, influences, and willingness to be involved in Medical Assistance in Dying (MAiD): a mixed method modified e-Delphi study
- Jocelyn Schroeder 1 ,
- Barbara Pesut 1 , 2 ,
- Lise Olsen 2 ,
- Nelly D. Oelke 2 &
- Helen Sharp 2
BMC Nursing volume 23 , Article number: 326 ( 2024 ) Cite this article
31 Accesses
Metrics details
Medical Assistance in Dying (MAiD) was legalized in Canada in 2016. Canada’s legislation is the first to permit Nurse Practitioners (NP) to serve as independent MAiD assessors and providers. Registered Nurses’ (RN) also have important roles in MAiD that include MAiD care coordination; client and family teaching and support, MAiD procedural quality; healthcare provider and public education; and bereavement care for family. Nurses have a right under the law to conscientious objection to participating in MAiD. Therefore, it is essential to prepare nurses in their entry-level education for the practice implications and moral complexities inherent in this practice. Knowing what nursing students think about MAiD is a critical first step. Therefore, the purpose of this study was to develop a survey to measure nursing students’ knowledge, attitudes and beliefs, influences, and willingness to be involved in MAiD in the Canadian context.
The design was a mixed-method, modified e-Delphi method that entailed item generation from the literature, item refinement through a 2 round survey of an expert faculty panel, and item validation through a cognitive focus group interview with nursing students. The settings were a University located in an urban area and a College located in a rural area in Western Canada.
During phase 1, a 56-item survey was developed from existing literature that included demographic items and items designed to measure experience with death and dying (including MAiD), education and preparation, attitudes and beliefs, influences on those beliefs, and anticipated future involvement. During phase 2, an expert faculty panel reviewed, modified, and prioritized the items yielding 51 items. During phase 3, a sample of nursing students further evaluated and modified the language in the survey to aid readability and comprehension. The final survey consists of 45 items including 4 case studies.
Systematic evaluation of knowledge-to-date coupled with stakeholder perspectives supports robust survey design. This study yielded a survey to assess nursing students’ attitudes toward MAiD in a Canadian context.
The survey is appropriate for use in education and research to measure knowledge and attitudes about MAiD among nurse trainees and can be a helpful step in preparing nursing students for entry-level practice.
Peer Review reports
Medical Assistance in Dying (MAiD) is permitted under an amendment to Canada’s Criminal Code which was passed in 2016 [ 1 ]. MAiD is defined in the legislation as both self-administered and clinician-administered medication for the purpose of causing death. In the 2016 Bill C-14 legislation one of the eligibility criteria was that an applicant for MAiD must have a reasonably foreseeable natural death although this term was not defined. It was left to the clinical judgement of MAiD assessors and providers to determine the time frame that constitutes reasonably foreseeable [ 2 ]. However, in 2021 under Bill C-7, the eligibility criteria for MAiD were changed to allow individuals with irreversible medical conditions, declining health, and suffering, but whose natural death was not reasonably foreseeable, to receive MAiD [ 3 ]. This population of MAiD applicants are referred to as Track 2 MAiD (those whose natural death is foreseeable are referred to as Track 1). Track 2 applicants are subject to additional safeguards under the 2021 C-7 legislation.
Three additional proposed changes to the legislation have been extensively studied by Canadian Expert Panels (Council of Canadian Academics [CCA]) [ 4 , 5 , 6 ] First, under the legislation that defines Track 2, individuals with mental disease as their sole underlying medical condition may apply for MAiD, but implementation of this practice is embargoed until March 2027 [ 4 ]. Second, there is consideration of allowing MAiD to be implemented through advanced consent. This would make it possible for persons living with dementia to receive MAID after they have lost the capacity to consent to the procedure [ 5 ]. Third, there is consideration of extending MAiD to mature minors. A mature minor is defined as “a person under the age of majority…and who has the capacity to understand and appreciate the nature and consequences of a decision” ([ 6 ] p. 5). In summary, since the legalization of MAiD in 2016 the eligibility criteria and safeguards have evolved significantly with consequent implications for nurses and nursing care. Further, the number of Canadians who access MAiD shows steady increases since 2016 [ 7 ] and it is expected that these increases will continue in the foreseeable future.
Nurses have been integral to MAiD care in the Canadian context. While other countries such as Belgium and the Netherlands also permit euthanasia, Canada is the first country to allow Nurse Practitioners (Registered Nurses with additional preparation typically achieved at the graduate level) to act independently as assessors and providers of MAiD [ 1 ]. Although the role of Registered Nurses (RNs) in MAiD is not defined in federal legislation, it has been addressed at the provincial/territorial-level with variability in scope of practice by region [ 8 , 9 ]. For example, there are differences with respect to the obligation of the nurse to provide information to patients about MAiD, and to the degree that nurses are expected to ensure that patient eligibility criteria and safeguards are met prior to their participation [ 10 ]. Studies conducted in the Canadian context indicate that RNs perform essential roles in MAiD care coordination; client and family teaching and support; MAiD procedural quality; healthcare provider and public education; and bereavement care for family [ 9 , 11 ]. Nurse practitioners and RNs are integral to a robust MAiD care system in Canada and hence need to be well-prepared for their role [ 12 ].
Previous studies have found that end of life care, and MAiD specifically, raise complex moral and ethical issues for nurses [ 13 , 14 , 15 , 16 ]. The knowledge, attitudes, and beliefs of nurses are important across practice settings because nurses have consistent, ongoing, and direct contact with patients who experience chronic or life-limiting health conditions. Canadian studies exploring nurses’ moral and ethical decision-making in relation to MAiD reveal that although some nurses are clear in their support for, or opposition to, MAiD, others are unclear on what they believe to be good and right [ 14 ]. Empirical findings suggest that nurses go through a period of moral sense-making that is often informed by their family, peers, and initial experiences with MAID [ 17 , 18 ]. Canadian legislation and policy specifies that nurses are not required to participate in MAiD and may recuse themselves as conscientious objectors with appropriate steps to ensure ongoing and safe care of patients [ 1 , 19 ]. However, with so many nurses having to reflect on and make sense of their moral position, it is essential that they are given adequate time and preparation to make an informed and thoughtful decision before they participate in a MAID death [ 20 , 21 ].
It is well established that nursing students receive inconsistent exposure to end of life care issues [ 22 ] and little or no training related to MAiD [ 23 ]. Without such education and reflection time in pre-entry nursing preparation, nurses are at significant risk for moral harm. An important first step in providing this preparation is to be able to assess the knowledge, values, and beliefs of nursing students regarding MAID and end of life care. As demand for MAiD increases along with the complexities of MAiD, it is critical to understand the knowledge, attitudes, and likelihood of engagement with MAiD among nursing students as a baseline upon which to build curriculum and as a means to track these variables over time.
Aim, design, and setting
The aim of this study was to develop a survey to measure nursing students’ knowledge, attitudes and beliefs, influences, and willingness to be involved in MAiD in the Canadian context. We sought to explore both their willingness to be involved in the registered nursing role and in the nurse practitioner role should they chose to prepare themselves to that level of education. The design was a mixed-method, modified e-Delphi method that entailed item generation, item refinement through an expert faculty panel [ 24 , 25 , 26 ], and initial item validation through a cognitive focus group interview with nursing students [ 27 ]. The settings were a University located in an urban area and a College located in a rural area in Western Canada.
Participants
A panel of 10 faculty from the two nursing education programs were recruited for Phase 2 of the e-Delphi. To be included, faculty were required to have a minimum of three years of experience in nurse education, be employed as nursing faculty, and self-identify as having experience with MAiD. A convenience sample of 5 fourth-year nursing students were recruited to participate in Phase 3. Students had to be in good standing in the nursing program and be willing to share their experiences of the survey in an online group interview format.
The modified e-Delphi was conducted in 3 phases: Phase 1 entailed item generation through literature and existing survey review. Phase 2 entailed item refinement through a faculty expert panel review with focus on content validity, prioritization, and revision of item wording [ 25 ]. Phase 3 entailed an assessment of face validity through focus group-based cognitive interview with nursing students.
Phase I. Item generation through literature review
The goal of phase 1 was to develop a bank of survey items that would represent the variables of interest and which could be provided to expert faculty in Phase 2. Initial survey items were generated through a literature review of similar surveys designed to assess knowledge and attitudes toward MAiD/euthanasia in healthcare providers; Canadian empirical studies on nurses’ roles and/or experiences with MAiD; and legislative and expert panel documents that outlined proposed changes to the legislative eligibility criteria and safeguards. The literature review was conducted in three online databases: CINAHL, PsycINFO, and Medline. Key words for the search included nurses , nursing students , medical students , NPs, MAiD , euthanasia , assisted death , and end-of-life care . Only articles written in English were reviewed. The legalization and legislation of MAiD is new in many countries; therefore, studies that were greater than twenty years old were excluded, no further exclusion criteria set for country.
Items from surveys designed to measure similar variables in other health care providers and geographic contexts were placed in a table and similar items were collated and revised into a single item. Then key variables were identified from the empirical literature on nurses and MAiD in Canada and checked against the items derived from the surveys to ensure that each of the key variables were represented. For example, conscientious objection has figured prominently in the Canadian literature, but there were few items that assessed knowledge of conscientious objection in other surveys and so items were added [ 15 , 21 , 28 , 29 ]. Finally, four case studies were added to the survey to address the anticipated changes to the Canadian legislation. The case studies were based upon the inclusion of mature minors, advanced consent, and mental disorder as the sole underlying medical condition. The intention was to assess nurses’ beliefs and comfort with these potential legislative changes.
Phase 2. Item refinement through expert panel review
The goal of phase 2 was to refine and prioritize the proposed survey items identified in phase 1 using a modified e-Delphi approach to achieve consensus among an expert panel [ 26 ]. Items from phase 1 were presented to an expert faculty panel using a Qualtrics (Provo, UT) online survey. Panel members were asked to review each item to determine if it should be: included, excluded or adapted for the survey. When adapted was selected faculty experts were asked to provide rationale and suggestions for adaptation through the use of an open text box. Items that reached a level of 75% consensus for either inclusion or adaptation were retained [ 25 , 26 ]. New items were categorized and added, and a revised survey was presented to the panel of experts in round 2. Panel members were again asked to review items, including new items, to determine if it should be: included, excluded, or adapted for the survey. Round 2 of the modified e-Delphi approach also included an item prioritization activity, where participants were then asked to rate the importance of each item, based on a 5-point Likert scale (low to high importance), which De Vaus [ 30 ] states is helpful for increasing the reliability of responses. Items that reached a 75% consensus on inclusion were then considered in relation to the importance it was given by the expert panel. Quantitative data were managed using SPSS (IBM Corp).
Phase 3. Face validity through cognitive interviews with nursing students
The goal of phase 3 was to obtain initial face validity of the proposed survey using a sample of nursing student informants. More specifically, student participants were asked to discuss how items were interpreted, to identify confusing wording or other problematic construction of items, and to provide feedback about the survey as a whole including readability and organization [ 31 , 32 , 33 ]. The focus group was held online and audio recorded. A semi-structured interview guide was developed for this study that focused on clarity, meaning, order and wording of questions; emotions evoked by the questions; and overall survey cohesion and length was used to obtain data (see Supplementary Material 2 for the interview guide). A prompt to “think aloud” was used to limit interviewer-imposed bias and encourage participants to describe their thoughts and response to a given item as they reviewed survey items [ 27 ]. Where needed, verbal probes such as “could you expand on that” were used to encourage participants to expand on their responses [ 27 ]. Student participants’ feedback was collated verbatim and presented to the research team where potential survey modifications were negotiated and finalized among team members. Conventional content analysis [ 34 ] of focus group data was conducted to identify key themes that emerged through discussion with students. Themes were derived from the data by grouping common responses and then using those common responses to modify survey items.
Ten nursing faculty participated in the expert panel. Eight of the 10 faculty self-identified as female. No faculty panel members reported conscientious objector status and ninety percent reported general agreement with MAiD with one respondent who indicated their view as “unsure.” Six of the 10 faculty experts had 16 years of experience or more working as a nurse educator.
Five nursing students participated in the cognitive interview focus group. The duration of the focus group was 2.5 h. All participants identified that they were born in Canada, self-identified as female (one preferred not to say) and reported having received some instruction about MAiD as part of their nursing curriculum. See Tables 1 and 2 for the demographic descriptors of the study sample. Study results will be reported in accordance with the study phases. See Fig. 1 for an overview of the results from each phase.

Fig. 1 Overview of survey development findings
Phase 1: survey item generation
Review of the literature identified that no existing survey was available for use with nursing students in the Canadian context. However, an analysis of themes across qualitative and quantitative studies of physicians, medical students, nurses, and nursing students provided sufficient data to develop a preliminary set of items suitable for adaptation to a population of nursing students.
Four major themes and factors that influence knowledge, attitudes, and beliefs about MAiD were evident from the literature: (i) endogenous or individual factors such as age, gender, personally held values, religion, religiosity, and/or spirituality [ 35 , 36 , 37 , 38 , 39 , 40 , 41 , 42 ], (ii) experience with death and dying in personal and/or professional life [ 35 , 40 , 41 , 43 , 44 , 45 ], (iii) training including curricular instruction about clinical role, scope of practice, or the law [ 23 , 36 , 39 ], and (iv) exogenous or social factors such as the influence of key leaders, colleagues, friends and/or family, professional and licensure organizations, support within professional settings, and/or engagement in MAiD in an interdisciplinary team context [ 9 , 35 , 46 ].
Studies of nursing students also suggest overlap across these categories. For example, value for patient autonomy [ 23 ] and the moral complexity of decision-making [ 37 ] are important factors that contribute to attitudes about MAiD and may stem from a blend of personally held values coupled with curricular content, professional training and norms, and clinical exposure. For example, students report that participation in end of life care allows for personal growth, shifts in perception, and opportunities to build therapeutic relationships with their clients [ 44 , 47 , 48 ].
Preliminary items generated from the literature resulted in 56 questions from 11 published sources (See Table 3 ). These items were constructed across four main categories: (i) socio-demographic questions; (ii) end of life care questions; (iii) knowledge about MAiD; or (iv) comfort and willingness to participate in MAiD. Knowledge questions were refined to reflect current MAiD legislation, policies, and regulatory frameworks. Falconer [ 39 ] and Freeman [ 45 ] studies were foundational sources for item selection. Additionally, four case studies were written to reflect the most recent anticipated changes to MAiD legislation and all used the same open-ended core questions to address respondents’ perspectives about the patient’s right to make the decision, comfort in assisting a physician or NP to administer MAiD in that scenario, and hypothesized comfort about serving as a primary provider if qualified as an NP in future. Response options for the survey were also constructed during this stage and included: open text, categorical, yes/no , and Likert scales.
Phase 2: faculty expert panel review
Of the 56 items presented to the faculty panel, 54 questions reached 75% consensus. However, based upon the qualitative responses 9 items were removed largely because they were felt to be repetitive. Items that generated the most controversy were related to measuring religion and spirituality in the Canadian context, defining end of life care when there is no agreed upon time frames (e.g., last days, months, or years), and predicting willingness to be involved in a future events – thus predicting their future selves. Phase 2, round 1 resulted in an initial set of 47 items which were then presented back to the faculty panel in round 2.
Of the 47 initial questions presented to the panel in round 2, 45 reached a level of consensus of 75% or greater, and 34 of these questions reached a level of 100% consensus [ 27 ] of which all participants chose to include without any adaptations) For each question, level of importance was determined based on a 5-point Likert scale (1 = very unimportant, 2 = somewhat unimportant, 3 = neutral, 4 = somewhat important, and 5 = very important). Figure 2 provides an overview of the level of importance assigned to each item.

Ranking level of importance for survey items
After round 2, a careful analysis of participant comments and level of importance was completed by the research team. While the main method of survey item development came from participants’ response to the first round of Delphi consensus ratings, level of importance was used to assist in the decision of whether to keep or modify questions that created controversy, or that rated lower in the include/exclude/adapt portion of the Delphi. Survey items that rated low in level of importance included questions about future roles, sex and gender, and religion/spirituality. After deliberation by the research committee, these questions were retained in the survey based upon the importance of these variables in the scientific literature.
Of the 47 questions remaining from Phase 2, round 2, four were revised. In addition, the two questions that did not meet the 75% cut off level for consensus were reviewed by the research team. The first question reviewed was What is your comfort level with providing a MAiD death in the future if you were a qualified NP ? Based on a review of participant comments, it was decided to retain this question for the cognitive interviews with students in the final phase of testing. The second question asked about impacts on respondents’ views of MAiD and was changed from one item with 4 subcategories into 4 separate items, resulting in a final total of 51 items for phase 3. The revised survey was then brought forward to the cognitive interviews with student participants in Phase 3. (see Supplementary Material 1 for a complete description of item modification during round 2).
Phase 3. Outcomes of cognitive interview focus group
Of the 51 items reviewed by student participants, 29 were identified as clear with little or no discussion. Participant comments for the remaining 22 questions were noted and verified against the audio recording. Following content analysis of the comments, four key themes emerged through the student discussion: unclear or ambiguous wording; difficult to answer questions; need for additional response options; and emotional response evoked by questions. An example of unclear or ambiguous wording was a request for clarity in the use of the word “sufficient” in the context of assessing an item that read “My nursing education has provided sufficient content about the nursing role in MAiD.” “Sufficient” was viewed as subjective and “laden with…complexity that distracted me from the question.” The group recommended rewording the item to read “My nursing education has provided enough content for me to care for a patient considering or requesting MAiD.”
An example of having difficulty answering questions related to limited knowledge related to terms used in the legislation such as such as safeguards , mature minor , eligibility criteria , and conscientious objection. Students were unclear about what these words meant relative to the legislation and indicated that this lack of clarity would hamper appropriate responses to the survey. To ensure that respondents are able to answer relevant questions, student participants recommended that the final survey include explanation of key terms such as mature minor and conscientious objection and an overview of current legislation.
Response options were also a point of discussion. Participants noted a lack of distinction between response options of unsure and unable to say . Additionally, scaling of attitudes was noted as important since perspectives about MAiD are dynamic and not dichotomous “agree or disagree” responses. Although the faculty expert panel recommended the integration of the demographic variables of religious and/or spiritual remain as a single item, the student group stated a preference to have religion and spirituality appear as separate items. The student focus group also took issue with separate items for the variables of sex and gender, specifically that non-binary respondents might feel othered or “outed” particularly when asked to identify their sex. These variables had been created based upon best practices in health research but students did not feel they were appropriate in this context [ 49 ]. Finally, students agreed with the faculty expert panel in terms of the complexity of projecting their future involvement as a Nurse Practitioner. One participant stated: “I certainly had to like, whoa, whoa, whoa. Now let me finish this degree first, please.” Another stated, “I'm still imagining myself, my future career as an RN.”
Finally, student participants acknowledged the array of emotions that some of the items produced for them. For example, one student described positive feelings when interacting with the survey. “Brought me a little bit of feeling of joy. Like it reminded me that this is the last piece of independence that people grab on to.” Another participant, described the freedom that the idea of an advance request gave her. “The advance request gives the most comfort for me, just with early onset Alzheimer’s and knowing what it can do.” But other participants described less positive feelings. For example, the mature minor case study yielded a comment: “This whole scenario just made my heart hurt with the idea of a child requesting that.”
Based on the data gathered from the cognitive interview focus group of nursing students, revisions were made to 11 closed-ended questions (see Table 4 ) and 3 items were excluded. In the four case studies, the open-ended question related to a respondents’ hypothesized actions in a future role as NP were removed. The final survey consists of 45 items including 4 case studies (see Supplementary Material 3 ).
The aim of this study was to develop and validate a survey that can be used to track the growth of knowledge about MAiD among nursing students over time, inform training programs about curricular needs, and evaluate attitudes and willingness to participate in MAiD at time-points during training or across nursing programs over time.
The faculty expert panel and student participants in the cognitive interview focus group identified a need to establish core knowledge of the terminology and legislative rules related to MAiD. For example, within the cognitive interview group of student participants, several acknowledged lack of clear understanding of specific terms such as “conscientious objector” and “safeguards.” Participants acknowledged discomfort with the uncertainty of not knowing and their inclination to look up these terms to assist with answering the questions. This survey can be administered to nursing or pre-nursing students at any phase of their training within a program or across training programs. However, in doing so it is important to acknowledge that their baseline knowledge of MAiD will vary. A response option of “not sure” is important and provides a means for respondents to convey uncertainty. If this survey is used to inform curricular needs, respondents should be given explicit instructions not to conduct online searches to inform their responses, but rather to provide an honest appraisal of their current knowledge and these instructions are included in the survey (see Supplementary Material 3 ).
Some provincial regulatory bodies have established core competencies for entry-level nurses that include MAiD. For example, the BC College of Nurses and Midwives (BCCNM) requires “knowledge about ethical, legal, and regulatory implications of medical assistance in dying (MAiD) when providing nursing care.” (10 p. 6) However, across Canada curricular content and coverage related to end of life care and MAiD is variable [ 23 ]. Given the dynamic nature of the legislation that includes portions of the law that are embargoed until 2024, it is important to ensure that respondents are guided by current and accurate information. As the law changes, nursing curricula, and public attitudes continue to evolve, inclusion of core knowledge and content is essential and relevant for investigators to be able to interpret the portions of the survey focused on attitudes and beliefs about MAiD. Content knowledge portions of the survey may need to be modified over time as legislation and training change and to meet the specific purposes of the investigator.
Given the sensitive nature of the topic, it is strongly recommended that surveys be conducted anonymously and that students be provided with an opportunity to discuss their responses to the survey. A majority of feedback from both the expert panel of faculty and from student participants related to the wording and inclusion of demographic variables, in particular religion, religiosity, gender identity, and sex assigned at birth. These and other demographic variables have the potential to be highly identifying in small samples. In any instance in which the survey could be expected to yield demographic group sizes less than 5, users should eliminate the demographic variables from the survey. For example, the profession of nursing is highly dominated by females with over 90% of nurses who identify as female [ 50 ]. Thus, a survey within a single class of students or even across classes in a single institution is likely to yield a small number of male respondents and/or respondents who report a difference between sex assigned at birth and gender identity. When variables that serve to identify respondents are included, respondents are less likely to complete or submit the survey, to obscure their responses so as not to be identifiable, or to be influenced by social desirability bias in their responses rather than to convey their attitudes accurately [ 51 ]. Further, small samples do not allow for conclusive analyses or interpretation of apparent group differences. Although these variables are often included in surveys, such demographics should be included only when anonymity can be sustained. In small and/or known samples, highly identifying variables should be omitted.
There are several limitations associated with the development of this survey. The expert panel was comprised of faculty who teach nursing students and are knowledgeable about MAiD and curricular content, however none identified as a conscientious objector to MAiD. Ideally, our expert panel would have included one or more conscientious objectors to MAiD to provide a broader perspective. Review by practitioners who participate in MAiD, those who are neutral or undecided, and practitioners who are conscientious objectors would ensure broad applicability of the survey. This study included one student cognitive interview focus group with 5 self-selected participants. All student participants had held discussions about end of life care with at least one patient, 4 of 5 participants had worked with a patient who requested MAiD, and one had been present for a MAiD death. It is not clear that these participants are representative of nursing students demographically or by experience with end of life care. It is possible that the students who elected to participate hold perspectives and reflections on patient care and MAiD that differ from students with little or no exposure to end of life care and/or MAiD. However, previous studies find that most nursing students have been involved with end of life care including meaningful discussions about patients’ preferences and care needs during their education [ 40 , 44 , 47 , 48 , 52 ]. Data collection with additional student focus groups with students early in their training and drawn from other training contexts would contribute to further validation of survey items.
Future studies should incorporate pilot testing with small sample of nursing students followed by a larger cross-program sample to allow evaluation of the psychometric properties of specific items and further refinement of the survey tool. Consistent with literature about the importance of leadership in the context of MAiD [ 12 , 53 , 54 ], a study of faculty knowledge, beliefs, and attitudes toward MAiD would provide context for understanding student perspectives within and across programs. Additional research is also needed to understand the timing and content coverage of MAiD across Canadian nurse training programs’ curricula.
The implementation of MAiD is complex and requires understanding of the perspectives of multiple stakeholders. Within the field of nursing this includes clinical providers, educators, and students who will deliver clinical care. A survey to assess nursing students’ attitudes toward and willingness to participate in MAiD in the Canadian context is timely, due to the legislation enacted in 2016 and subsequent modifications to the law in 2021 with portions of the law to be enacted in 2027. Further development of this survey could be undertaken to allow for use in settings with practicing nurses or to allow longitudinal follow up with students as they enter practice. As the Canadian landscape changes, ongoing assessment of the perspectives and needs of health professionals and students in the health professions is needed to inform policy makers, leaders in practice, curricular needs, and to monitor changes in attitudes and practice patterns over time.
Availability of data and materials
The datasets used and/or analysed during the current study are not publicly available due to small sample sizes, but are available from the corresponding author on reasonable request.
Abbreviations
British Columbia College of Nurses and Midwives
Medical assistance in dying
Nurse practitioner
Registered nurse
University of British Columbia Okanagan
Nicol J, Tiedemann M. Legislative Summary: Bill C-14: An Act to amend the Criminal Code and to make related amendments to other Acts (medical assistance in dying). Available from: https://lop.parl.ca/staticfiles/PublicWebsite/Home/ResearchPublications/LegislativeSummaries/PDF/42-1/c14-e.pdf .
Downie J, Scallion K. Foreseeably unclear. The meaning of the “reasonably foreseeable” criterion for access to medical assistance in dying in Canada. Dalhousie Law J. 2018;41(1):23–57.
Nicol J, Tiedeman M. Legislative summary of Bill C-7: an act to amend the criminal code (medical assistance in dying). Ottawa: Government of Canada; 2021.
Google Scholar
Council of Canadian Academies. The state of knowledge on medical assistance in dying where a mental disorder is the sole underlying medical condition. Ottawa; 2018. Available from: https://cca-reports.ca/wp-content/uploads/2018/12/The-State-of-Knowledge-on-Medical-Assistance-in-Dying-Where-a-Mental-Disorder-is-the-Sole-Underlying-Medical-Condition.pdf .
Council of Canadian Academies. The state of knowledge on advance requests for medical assistance in dying. Ottawa; 2018. Available from: https://cca-reports.ca/wp-content/uploads/2019/02/The-State-of-Knowledge-on-Advance-Requests-for-Medical-Assistance-in-Dying.pdf .
Council of Canadian Academies. The state of knowledge on medical assistance in dying for mature minors. Ottawa; 2018. Available from: https://cca-reports.ca/wp-content/uploads/2018/12/The-State-of-Knowledge-on-Medical-Assistance-in-Dying-for-Mature-Minors.pdf .
Health Canada. Third annual report on medical assistance in dying in Canada 2021. Ottawa; 2022. [cited 2023 Oct 23]. Available from: https://www.canada.ca/en/health-canada/services/medical-assistance-dying/annual-report-2021.html .
Banner D, Schiller CJ, Freeman S. Medical assistance in dying: a political issue for nurses and nursing in Canada. Nurs Philos. 2019;20(4): e12281.
Article PubMed Google Scholar
Pesut B, Thorne S, Stager ML, Schiller CJ, Penney C, Hoffman C, et al. Medical assistance in dying: a review of Canadian nursing regulatory documents. Policy Polit Nurs Pract. 2019;20(3):113–30.
Article PubMed PubMed Central Google Scholar
College of Registered Nurses of British Columbia. Scope of practice for registered nurses [Internet]. Vancouver; 2018. Available from: https://www.bccnm.ca/Documents/standards_practice/rn/RN_ScopeofPractice.pdf .
Pesut B, Thorne S, Schiller C, Greig M, Roussel J, Tishelman C. Constructing good nursing practice for medical assistance in dying in Canada: an interpretive descriptive study. Global Qual Nurs Res. 2020;7:2333393620938686. https://doi.org/10.1177/2333393620938686 .
Article Google Scholar
Pesut B, Thorne S, Schiller CJ, Greig M, Roussel J. The rocks and hard places of MAiD: a qualitative study of nursing practice in the context of legislated assisted death. BMC Nurs. 2020;19:12. https://doi.org/10.1186/s12912-020-0404-5 .
Pesut B, Greig M, Thorne S, Burgess M, Storch JL, Tishelman C, et al. Nursing and euthanasia: a narrative review of the nursing ethics literature. Nurs Ethics. 2020;27(1):152–67.
Pesut B, Thorne S, Storch J, Chambaere K, Greig M, Burgess M. Riding an elephant: a qualitative study of nurses’ moral journeys in the context of Medical Assistance in Dying (MAiD). Journal Clin Nurs. 2020;29(19–20):3870–81.
Lamb C, Babenko-Mould Y, Evans M, Wong CA, Kirkwood KW. Conscientious objection and nurses: results of an interpretive phenomenological study. Nurs Ethics. 2018;26(5):1337–49.
Wright DK, Chan LS, Fishman JR, Macdonald ME. “Reflection and soul searching:” Negotiating nursing identity at the fault lines of palliative care and medical assistance in dying. Social Sci & Med. 2021;289: 114366.
Beuthin R, Bruce A, Scaia M. Medical assistance in dying (MAiD): Canadian nurses’ experiences. Nurs Forum. 2018;54(4):511–20.
Bruce A, Beuthin R. Medically assisted dying in Canada: "Beautiful Death" is transforming nurses' experiences of suffering. The Canadian J Nurs Res | Revue Canadienne de Recherche en Sci Infirmieres. 2020;52(4):268–77. https://doi.org/10.1177/0844562119856234 .
Canadian Nurses Association. Code of ethics for registered nurses. Ottawa; 2017. Available from: https://www.cna-aiic.ca/en/nursing/regulated-nursing-in-canada/nursing-ethics .
Canadian Nurses Association. National nursing framework on Medical Assistance in Dying in Canada. Ottawa: 2017. Available from: https://www.virtualhospice.ca/Assets/cna-national-nursing-framework-on-maidEng_20170216155827.pdf .
Pesut B, Thorne S, Greig M. Shades of gray: conscientious objection in medical assistance in dying. Nursing Inq. 2020;27(1): e12308.
Durojaiye A, Ryan R, Doody O. Student nurse education and preparation for palliative care: a scoping review. PLoS ONE. 2023. https://doi.org/10.1371/journal.pone.0286678 .
McMechan C, Bruce A, Beuthin R. Canadian nursing students’ experiences with medical assistance in dying | Les expériences d’étudiantes en sciences infirmières au regard de l’aide médicale à mourir. Qual Adv Nurs Educ - Avancées en Formation Infirmière. 2019;5(1). https://doi.org/10.17483/2368-6669.1179 .
Adler M, Ziglio E. Gazing into the oracle. The Delphi method and its application to social policy and public health. London: Jessica Kingsley Publishers; 1996
Keeney S, Hasson F, McKenna H. Consulting the oracle: ten lessons from using the Delphi technique in nursing research. J Adv Nurs. 2006;53(2):205–12.
Keeney S, Hasson F, McKenna H. The Delphi technique in nursing and health research. 1st ed. City: Wiley; 2011.
Willis GB. Cognitive interviewing: a tool for improving questionnaire design. 1st ed. Thousand Oaks, Calif: Sage; 2005. ISBN: 9780761928041
Lamb C, Evans M, Babenko-Mould Y, Wong CA, Kirkwood EW. Conscience, conscientious objection, and nursing: a concept analysis. Nurs Ethics. 2017;26(1):37–49.
Lamb C, Evans M, Babenko-Mould Y, Wong CA, Kirkwood K. Nurses’ use of conscientious objection and the implications of conscience. J Adv Nurs. 2018;75(3):594–602.
de Vaus D. Surveys in social research. 6th ed. Abingdon, Oxon: Routledge; 2014.
Boateng GO, Neilands TB, Frongillo EA, Melgar-Quiñonez HR, Young SL. Best practices for developing and validating scales for health, social, and behavioral research: A primer. Front Public Health. 2018;6:149. https://doi.org/10.3389/fpubh.2018.00149 .
Puchta C, Potter J. Focus group practice. 1st ed. London: Sage; 2004.
Book Google Scholar
Streiner DL, Norman GR, Cairney J. Health measurement scales: a practical guide to their development and use. 5th ed. Oxford: Oxford University Press; 2015.
Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88.
Adesina O, DeBellis A, Zannettino L. Third-year Australian nursing students’ attitudes, experiences, knowledge, and education concerning end-of-life care. Int J of Palliative Nurs. 2014;20(8):395–401.
Bator EX, Philpott B, Costa AP. This moral coil: a cross-sectional survey of Canadian medical student attitudes toward medical assistance in dying. BMC Med Ethics. 2017;18(1):58.
Beuthin R, Bruce A, Scaia M. Medical assistance in dying (MAiD): Canadian nurses’ experiences. Nurs Forum. 2018;53(4):511–20.
Brown J, Goodridge D, Thorpe L, Crizzle A. What is right for me, is not necessarily right for you: the endogenous factors influencing nonparticipation in medical assistance in dying. Qual Health Res. 2021;31(10):1786–1800.
Falconer J, Couture F, Demir KK, Lang M, Shefman Z, Woo M. Perceptions and intentions toward medical assistance in dying among Canadian medical students. BMC Med Ethics. 2019;20(1):22.
Green G, Reicher S, Herman M, Raspaolo A, Spero T, Blau A. Attitudes toward euthanasia—dual view: Nursing students and nurses. Death Stud. 2022;46(1):124–31.
Hosseinzadeh K, Rafiei H. Nursing student attitudes toward euthanasia: a cross-sectional study. Nurs Ethics. 2019;26(2):496–503.
Ozcelik H, Tekir O, Samancioglu S, Fadiloglu C, Ozkara E. Nursing students’ approaches toward euthanasia. Omega (Westport). 2014;69(1):93–103.
Canning SE, Drew C. Canadian nursing students’ understanding, and comfort levels related to medical assistance in dying. Qual Adv Nurs Educ - Avancées en Formation Infirmière. 2022;8(2). https://doi.org/10.17483/2368-6669.1326 .
Edo-Gual M, Tomás-Sábado J, Bardallo-Porras D, Monforte-Royo C. The impact of death and dying on nursing students: an explanatory model. J Clin Nurs. 2014;23(23–24):3501–12.
Freeman LA, Pfaff KA, Kopchek L, Liebman J. Investigating palliative care nurse attitudes towards medical assistance in dying: an exploratory cross-sectional study. J Adv Nurs. 2020;76(2):535–45.
Brown J, Goodridge D, Thorpe L, Crizzle A. “I am okay with it, but I am not going to do it:” the exogenous factors influencing non-participation in medical assistance in dying. Qual Health Res. 2021;31(12):2274–89.
Dimoula M, Kotronoulas G, Katsaragakis S, Christou M, Sgourou S, Patiraki E. Undergraduate nursing students’ knowledge about palliative care and attitudes towards end-of-life care: A three-cohort, cross-sectional survey. Nurs Educ Today. 2019;74:7–14.
Matchim Y, Raetong P. Thai nursing students’ experiences of caring for patients at the end of life: a phenomenological study. Int J Palliative Nurs. 2018;24(5):220–9.
Canadian Institute for Health Research. Sex and gender in health research [Internet]. Ottawa: CIHR; 2021 [cited 2023 Oct 23]. Available from: https://cihr-irsc.gc.ca/e/50833.html .
Canadian Nurses’ Association. Nursing statistics. Ottawa: CNA; 2023 [cited 2023 Oct 23]. Available from: https://www.cna-aiic.ca/en/nursing/regulated-nursing-in-canada/nursing-statistics .
Krumpal I. Determinants of social desirability bias in sensitive surveys: a literature review. Qual Quant. 2013;47(4):2025–47. https://doi.org/10.1007/s11135-011-9640-9 .
Ferri P, Di Lorenzo R, Stifani S, Morotti E, Vagnini M, Jiménez Herrera MF, et al. Nursing student attitudes toward dying patient care: a European multicenter cross-sectional study. Acta Bio Medica Atenei Parmensis. 2021;92(S2): e2021018.
PubMed PubMed Central Google Scholar
Beuthin R, Bruce A. Medical assistance in dying (MAiD): Ten things leaders need to know. Nurs Leadership. 2018;31(4):74–81.
Thiele T, Dunsford J. Nurse leaders’ role in medical assistance in dying: a relational ethics approach. Nurs Ethics. 2019;26(4):993–9.
Download references
Acknowledgements
We would like to acknowledge the faculty and students who generously contributed their time to this work.
JS received a student traineeship through the Principal Research Chairs program at the University of British Columbia Okanagan.
Author information
Authors and affiliations.
School of Health and Human Services, Selkirk College, Castlegar, BC, Canada
Jocelyn Schroeder & Barbara Pesut
School of Nursing, University of British Columbia Okanagan, Kelowna, BC, Canada
Barbara Pesut, Lise Olsen, Nelly D. Oelke & Helen Sharp
You can also search for this author in PubMed Google Scholar
Contributions
JS made substantial contributions to the conception of the work; data acquisition, analysis, and interpretation; and drafting and substantively revising the work. JS has approved the submitted version and agreed to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature. BP made substantial contributions to the conception of the work; data acquisition, analysis, and interpretation; and drafting and substantively revising the work. BP has approved the submitted version and agreed to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature. LO made substantial contributions to the conception of the work; data acquisition, analysis, and interpretation; and substantively revising the work. LO has approved the submitted version and agreed to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature. NDO made substantial contributions to the conception of the work; data acquisition, analysis, and interpretation; and substantively revising the work. NDO has approved the submitted version and agreed to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature. HS made substantial contributions to drafting and substantively revising the work. HS has approved the submitted version and agreed to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Authors’ information
JS conducted this study as part of their graduate requirements in the School of Nursing, University of British Columbia Okanagan.
Corresponding author
Correspondence to Barbara Pesut .
Ethics declarations
Ethics approval and consent to participate.
The research was approved by the Selkirk College Research Ethics Board (REB) ID # 2021–011 and the University of British Columbia Behavioral Research Ethics Board ID # H21-01181.
All participants provided written and informed consent through approved consent processes. Research was conducted in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare they have no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary material 1., supplementary material 2., supplementary material 3., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Schroeder, J., Pesut, B., Olsen, L. et al. Developing a survey to measure nursing students’ knowledge, attitudes and beliefs, influences, and willingness to be involved in Medical Assistance in Dying (MAiD): a mixed method modified e-Delphi study. BMC Nurs 23 , 326 (2024). https://doi.org/10.1186/s12912-024-01984-z
Download citation
Received : 24 October 2023
Accepted : 28 April 2024
Published : 14 May 2024
DOI : https://doi.org/10.1186/s12912-024-01984-z
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Medical assistance in dying (MAiD)
- End of life care
- Student nurses
- Nursing education
BMC Nursing
ISSN: 1472-6955
- General enquiries: [email protected]
Cross-Education of Muscular Endurance: A Scoping Review
- Review Article
- Open access
- Published: 17 May 2024
Cite this article
You have full access to this open access article

- Jun Seob Song 1 ,
- Yujiro Yamada 1 ,
- Ryo Kataoka 1 ,
- William B. Hammert 1 ,
- Anna Kang 1 &
- Jeremy P. Loenneke 1
7 Altmetric
It is well established that performing unilateral resistance training can increase muscle strength not only in the trained limb but also in the contralateral untrained limb, which is widely known as the cross-education of strength. However, less attention has been paid to the question of whether performing unilateral resistance training can induce cross-education of muscular endurance, despite its significant role in both athletic performance and activities of daily living.
The objectives of this scoping review were to provide an overview of the existing literature on cross-education of muscular endurance, as well as discuss its potential underlying mechanisms and offer considerations for future research.
A scoping review was conducted on the effects of unilateral resistance training on changes in muscular endurance in the contralateral untrained limb. This scoping review was conducted in PubMed, SPORTDiscus, and Scopus.
A total of 2000 articles were screened and 21 articles met the inclusion criteria. Among the 21 included studies, eight studies examined the cross-education of endurance via absolute ( n = 6) or relative ( n = 2) muscular endurance test, while five studies did not clearly indicate whether they examined absolute or relative muscular endurance. The remaining eight studies examined different types of muscular endurance measurements (e.g., time to task failure, total work, and fatigue index).
The current body of the literature does not provide sufficient evidence to draw clear conclusions on whether the cross-education of muscular endurance is present. The cross-education of muscular endurance (if it exists) may be potentially driven by neural adaptations (via bilateral access and/or cross-activation models that lead to cross-education of strength) and increased tolerance to exercise-induced discomfort. However, the limited number of available randomized controlled trials and the lack of understanding of underlying mechanisms provide a rationale for future research.
Avoid common mistakes on your manuscript.
1 Introduction
Resistance training leads to improvements in strength and muscular endurance [ 1 , 2 , 3 ]. When resistance training is performed on one side of the body only (i.e., unilateral resistance training), increased muscle strength has been observed not only in the trained limb but also in the contralateral untrained limb, which is widely known as the cross-education (or cross-transfer) of strength [ 4 , 5 ]. The cross-education of strength was first reported in the scientific literature as early as the late nineteenth century [ 6 ], and thereafter it has been studied and reviewed extensively over the years [ 4 , 5 , 7 , 8 , 9 ]. Although its underlying mechanisms are not entirely understood, there is a general consensus within the cross-education literature that the transfer of strength to the untrained limb is mediated primarily by neural mechanisms and likely not by mechanisms at the local muscle level (e.g., changes in muscle fiber type and cross-sectional area) as these changes appear to occur within the trained limb only [ 4 , 7 , 10 , 11 ]. In contrast to cross-education of strength, considerably less attention has been paid to the question of whether performing unilateral resistance training can increase muscular endurance in the contralateral untrained limb (i.e., cross-education of muscular endurance).
Muscular endurance refers to the ability of muscles to perform successive contractions at a submaximal load, and it is considered as an important physical fitness component not only for athletic performance in sports but also for activities of daily living that require repetitive work [ 12 ]. Muscular endurance can be further specified into absolute and relative muscular endurance [ 13 ]. Absolute muscular endurance involves performing a maximal number of repetitions with a given absolute load regardless of changes in maximal strength (e.g., using 60% of pretraining 1RM at pre- and posttesting) [ 14 ]. In contrast, relative muscular endurance involves an individual performing a maximal number of repetitions with a load corresponding to a specific relative intensity or percentage of the individual’s current 1RM (e.g., using 60% of pretraining and posttraining 1RM at pre- and posttesting, respectively) [ 14 ]. In addition, muscular endurance has been measured in several other ways when using different types of testing (e.g., isometric, isokinetic), such as time to task failure or total work during repeated isokinetic contractions [ 15 , 16 ]. There is evidence that resistance training can increase strength as well as induce positive mitochondrial and microvascular adaptations (e.g., mitochondrial respiratory capacity, capillary to fiber ratio), which may help explain muscular endurance adaptations in the trained limb [ 17 , 18 , 19 ]. However, it remains unclear whether these mechanisms can also explain the changes in muscular endurance in the contralateral untrained limb. Therefore, the purpose of this paper was to provide an overview of the existing literature on cross-education of muscular endurance following unilateral resistance training and to discuss its potential underlying mechanisms.
A scoping review was conducted to evaluate the cross-education of muscular endurance. The current study was conducted and reported in accordance with the Preferred Reporting for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) [ 20 ].
To identify relevant articles for the current scoping review, systematic literature searches were conducted from inception through April 2023, using PubMed, SPORTDiscus, and Scopus. Relevant studies were identified with the following search terms: “cross education” OR “cross transfer” OR “contralateral effect” OR “contralateral transfer” OR “interlimb transfer” OR “bilateral transfer” AND “endurance.” An additional search was carried out by examining the references of the included articles. Following the removal of duplicates, articles were screened first by title and abstract, followed by full text screening for eligibility. The study selection process is summarized using the PRISMA flow diagram (Fig. 1 ). In the present scoping review, broad inclusion criteria were used to provide an overview of the existing literature on cross-education of muscular endurance. To be included within the scoping review, studies were required to fulfill the following criteria: (1) original article was written in English language; (2) included a unilateral resistance exercise training intervention (regardless of strength training type and training load); (3) measured muscular endurance (e.g., number of repetitions at an absolute or relative load, time to task failure, total work) in the contralateral untrained limb at pre- and posttesting; and (4) was performed in humans with no restrictions on age and training status. One reviewer (JSS) completed literature searches and extraction of data. The following information was extracted: characteristics of participants, unilateral resistance training intervention (exercise type, sets, repetitions, load), frequency, duration, and main outcomes (cross-education of strength and muscular endurance). Two reviewers (JSS and JPL) checked the studies that only reported within-group changes (i.e., pre- to posttest) for each group, and back-calculated the p -value of between-group differences when possible.

Study selection process as per the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR)
3.1 Search Results
The systematic search provided 2000 articles (PubMed = 860, Scopus = 535, SPORTDiscus = 605), of which 377 were duplicates, leaving 1623 for screening. After title/abstract screening, 1516 articles were excluded and the remaining 107 articles were assessed for eligibility via full-text screening. Ninety-six articles were omitted following the full-text assessment, and 10 additional studies were included by reference checking. In total, 21 studies met the aforementioned criteria and were included in the review.
3.2 Study Characteristics
The present review included both randomized controlled trials and nonrandomized controlled trials. Of the 21 articles included in the review (Table 1 ), 10 studies were randomized controlled trials (including a nontraining control group) [ 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 ] and 11 studies were nonrandomized controlled trials [ 31 , 32 , 33 , 34 , 35 , 36 , 37 , 38 , 39 , 40 , 41 ]. Of note, this review focused more on randomized controlled trials, as it allows determination of whether changes in muscular endurance in an untrained limb (i.e., cross-education of muscular endurance) are solely due to the training interventions.
Among the 21 included studies, nine studies employed unilateral exercise training in the lower body (3 randomized controlled trials and 6 nonrandomized controlled trials) [ 21 , 23 , 24 , 31 , 33 , 35 , 36 , 37 , 39 ], nine studies in the upper arm (7 randomized controlled trials and 2 nonrandomized controlled trials) [ 22 , 25 , 26 , 27 , 28 , 29 , 30 , 40 , 41 ], and three studies used handgrip (3 nonrandomized controlled trials) [ 32 , 34 , 38 ]. For the muscular endurance measurements, absolute muscular endurance (i.e., number of repetitions with the same given load at pre- and postintervention, regardless of changes in maximal strength) was assessed in six studies [ 21 , 22 , 25 , 30 , 39 , 41 ], and relative muscular endurance (i.e., number of repetitions with a load corresponding to a specific relative intensity or percentage of individual’s current 1RM) was measured in two studies [ 26 , 27 ]. Of note, five studies did not provide enough detail to determine whether absolute or relative muscular endurance was examined for testing [ 23 , 29 , 32 , 38 , 40 ]. The remaining eight studies used several different types of muscular endurance measurements including: time to task failure (using absolute or relative load) [ 28 , 31 , 34 , 36 , 37 ], total work performed [ 24 , 33 ], and fatigue index (e.g., difference in work between the first three reps and the last three reps) [ 35 ]. Among the 21 included studies, five studies were conducted in untrained individuals [ 23 , 24 , 31 , 33 , 38 ], whereas the remaining 16 studies did not clearly describe the training status of the participants (e.g., physically active, college students from physical education program) [ 21 , 22 , 25 , 26 , 27 , 28 , 29 , 30 , 32 , 34 , 35 , 36 , 37 , 39 , 40 , 41 ].
4 Discussion
4.1 findings from nonrandomized controlled trials.
Several nonrandomized controlled trials reported changes in muscular endurance in the untrained limb following unilateral exercise training interventions. For example, 3 weeks of unilateral knee extension training increased absolute muscular endurance (i.e., maximal number of repetitions using 8.2 kg) in the contralateral untrained leg from pre- to posttest [ 39 ]. Similarly, 12 weeks of unilateral leg press exercise training increased relative muscular endurance [i.e., time to task failure during sustained isometric knee extension at relative 50% maximum voluntary isometric contraction (MVIC)] in the untrained leg from pre- to posttest [ 31 ]. In addition, four studies observed an increased muscular endurance (i.e., maximal number of repetitions and time to task failure) in the untrained limb (i.e., pre- to posttest) following 4–6 weeks of unilateral handgrip exercise training [ 32 , 34 , 38 ] and 6 weeks of unilateral isometric leg press training [ 37 ]. In those studies, however, it was unclear whether they used an absolute or relative muscular endurance test [ 32 , 34 , 37 , 38 ]. In one study, an increase in total work (i.e., during 30 maximum isokinetic knee extension) from pre- to posttest was observed in the untrained leg following 4 weeks of unilateral isokinetic knee extension and flexion [ 33 ]. However, these findings were not consistent throughout the literature. For example, no changes (i.e., pre- to posttest) in muscular endurance (i.e., absolute and/or relative, fatigue index) were observed in the contralateral untrained limb following unilateral knee extension training interventions [ 35 , 36 ], or following unilateral elbow flexion training interventions [ 40 , 41 ]. Of note, however, these findings should be interpreted with caution as it is not possible to know whether the changes in muscular endurance are due to the exercise training intervention or other factors outside of the training intervention. In other words, to determine whether the cross-education of muscular endurance is solely due to the training interventions, a time-matched nontraining control group is required (i.e., randomized controlled trials).
4.2 Findings from Randomized Controlled Trials
Among ten randomized controlled trials [ 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 ], three studies reported a cross-education of muscular endurance [ 23 , 30 ]. In male children (aged 10–13 years), for example, 8 weeks of unilateral leg press training increased not only strength but also muscular endurance (i.e., number of unilateral leg press repetitions with 60% of 1RM until failure) of the contralateral untrained leg compared with a nontraining control group [ 23 ]. In that study, however, it was not clear whether 60% of pre- or posttraining 1RM was used at the posttesting (i.e., absolute or relative muscular endurance) [ 23 ]. In healthy young males, 3 weeks of unilateral elbow flexion exercise training increased absolute muscular endurance (i.e., maximal number of unilateral elbow flexion repetitions with 6.4 kg) in the contralateral untrained arm compared with a nontraining control group [ 30 ]. In five randomized controlled trials, only within-group changes (i.e., pre- to posttest) in muscular endurance were reported [ 24 , 25 , 26 , 27 , 29 ]. For example, increases in muscular endurance (i.e., total work performed during 25 maximal isokinetic contractions and work performed during the last 5 repetitions) were observed in the contralateral untrained leg from pre- to posttest in a group that performed 7 weeks of isokinetic and isometric knee extension training, whereas no within-group changes were observed in a time-matched nontraining control group [ 24 ]. Similarly, increases in absolute and relative [ 25 , 26 ] muscular endurance from pre- to posttest were observed in the untrained arm following 6 weeks of unilateral elbow flexion training, while no changes were observed in a nontraining control group. In contrast, one study found no within-group changes (pre- to posttest) in either the training (i.e., 4 weeks of unilateral elbow flexion training) group or the nontraining control group [ 29 ]. Although some studies reported increases in muscular endurance only in the training groups and not in the control groups, this does not indicate that there was cross-education of muscular endurance. To determine whether a cross-education of muscular endurance is present, the changes in muscular endurance of the training groups should be directly compared with those of the control group. In one study, although only within-group changes (i.e., pre- to posttest) were reported for training and control groups, we were able to directly compare those two groups by back-calculating the p -value of between-group differences [ 27 ]. The calculation showed that the changes in relative muscular endurance in the untrained arm following 6 weeks of unilateral elbow flexion training were significantly greater compared with a control group, indicating a cross-education of relative muscular endurance [ 27 ]. Three randomized controlled trials did not observe cross-education of muscular endurance [ 21 , 22 , 28 ]. For example, no changes in absolute muscular endurance were observed in the contralateral untrained limb following 5 weeks of unilateral knee extension training [ 21 ] and following 5 weeks of unilateral elbow flexion training [ 22 ] when compared with a nontraining control group. Similarly, no changes in time to failure (i.e., sustaining at 100% MVIC until force drop below 50% MVIC) were observed in the untrained arm following 6 weeks of unilateral isometric elbow flexion training when compared with a nontraining control group [ 28 ].
Taken together, there is very limited evidence to suggest that performing unilateral resistance training can increase muscular endurance in the contralateral untrained limb (i.e., cross-education of muscular endurance). For example, there have been only three randomized controlled studies (out of 10 studies) that demonstrated evidence for cross-education of muscular endurance. Among these three studies, one showed increased absolute muscular endurance, another showed increased relative muscular endurance, and the third study showed increased muscular endurance (unclear whether absolute or relative). In contrast, the remaining seven studies either did not find or could not provide supporting evidence. These discrepancies in the cross-education of muscular endurance may be due to the differences in training interventions (e.g., contraction type, intensity, duration) and/or muscular endurance measurements (e.g., maximal number of repetitions and time to task failure using absolute or relative load). The current body of literature does not provide sufficient evidence to draw a clear conclusion on whether cross-education of muscular endurance is present, and thus requires further investigation.
4.3 Potential Underlying Mechanisms
There have been several mechanisms proposed to explain the increase in muscular endurance in the trained limb following resistance training, such as increased muscle capillarity [ 17 ] and mitochondrial respiratory capacity/function [ 42 , 43 ]. Although these proposed mechanisms may explain training-induced increases in muscular endurance in the trained limb, these would be unlikely to explain the changes in the contralateral untrained limb. The following section will discuss potential mechanisms that might contribute to the cross-education of muscular endurance.
4.3.1 Increases in Muscle Strength (Cross-Education of Strength)
One potential adaptation that could improve absolute muscular endurance in the contralateral untrained limb following unilateral resistance training is increased strength in the untrained limb via cross-education (i.e., cross-education of strength). According to the size principle, motor units are recruited in an orderly manner from the smaller motor units (i.e., low threshold) to the larger motor units (i.e., high threshold) as required force increases or muscle fatigues [ 44 ]. Based on this, increases in strength following resistance training may require fewer motor units to lift an absolute submaximal load for the same number of repetitions, which may delay the involvement of larger motor units and reserve them to be recruited subsequently for sustaining the required force as fatigue develops [ 14 , 45 ]. This hypothesis is partially supported by Ploutz et al. [ 45 ] who showed that less muscle was recruited to lift the same submaximal load in the untrained leg following 9 weeks of unilateral knee extension training [ 45 ], which may reserve larger motor units to be recruited later on and consequently allow for better performance on the absolute muscular endurance test in the untrained limb. However, this should be interpreted with caution since there was no time-matched control group, which makes it difficult to know whether the changes in muscle recruitment in the untrained limb were due to the unilateral training or some other factor [ 45 ]. The potential role of changes in strength on absolute muscular endurance may be also partially supported by a secondary analysis that examined if the changes in 1RM strength mediate changes in absolute muscular endurance (i.e., maximal number of repetitions using 42.5% pretraining 1RM) following high-load (i.e., 70% 1RM) training compared with low-load training interventions (i.e., 15% 1RM with or without blood flow restriction) [ 18 ]. In that study, it was found that training-induced increases in strength mediated the changes in muscular endurance in the high-load training group relative to the low-load training groups, suggesting that the differences in muscular endurance between high-load and low-load training groups may be explained by changes in strength. However, it is of note that the mediation analysis in that study only compared between training groups and not with a time-matched control group, meaning that the results can only explain the differences between training groups (i.e., high load versus low load). To clearly demonstrate whether the change in strength is an underlying mechanism for changes in muscular endurance, it may be more appropriate to compare training groups to a nonexercise control group in the mediation analysis. Furthermore, that analysis was on the changes in the trained limb, and thus it remains unknown whether increased strength from cross-education can also be translated to improved absolute muscular endurance in the untrained limb. One of the included studies reported concurrent increases in strength and muscular endurance in the untrained limb [ 23 ], whereas other studies showed that the cross-education of strength is not always accompanied by the cross-education of absolute muscular endurance [ 21 , 22 ]. Of note, simply assessing whether there were concurrent cross-education of strength and absolute muscular endurance may not be an appropriate approach to determine whether cross-education of strength can be translated to cross-education of absolute muscular endurance. A more appropriate approach might be using a mediation analysis to examine if the increases in strength from cross-education mediate the changes in absolute muscular endurance in the untrained limb [ 46 , 47 ]. It is of note that some previous studies have shown that unilateral low-load (or low-intensity) training does not increase strength in the opposite untrained limb (i.e., no cross-education of strength) [ 48 , 49 ]. However, this does not necessarily mean that unilateral low-load (or low-intensity) exercise would not induce cross-education of muscular endurance. It is plausible that cross-education of muscular endurance can occur in the absence of strength gain via different mechanisms.
4.3.2 Bilateral Access and Cross-Activation Model
Cross-education of relative muscular endurance likely cannot be explained by increased strength in the contralateral limb as relative muscular endurance is scaled to current maximal strength. Two main theoretical models, which may not be mutually exclusive, have been proposed to explain the cross-education of strength and skills: “bilateral access” and “cross-activation” models [ 50 ]. Although speculative, these two models may also explain the cross-education of muscular endurance. The “bilateral access” model involves the development of a motor engram during unilateral resistance training, which can be accessed not only by the trained limb, but also by the untrained limb for the control and execution of movements [ 50 , 51 ]. A widely used example is the “callosal access” hypothesis, in which the motor engrams developed in the trained hemisphere may be accessed by the opposite untrained hemisphere via the corpus callosum during motor tasks in the untrained limb [ 50 , 51 ]. In this model, it has been hypothesized that performing unilateral resistance training may develop an effective muscle recruitment pattern for maximum force production (i.e., muscle strength), such as coordination of synergists and inhibition of antagonists, which can be stored in neural circuits and accessed by the untrained hemisphere [ 4 ]. Although speculative, this hypothetical model may also play a role in the cross-education of muscular endurance. In other words, performing unilateral resistance training may create a motor engram of the motor output necessary to effectively perform repeated submaximal contractions, leading to cross-education of muscular endurance. However, further research is needed to determine whether or not the “bilateral access” model plays a role in the cross-education of muscular endurance in a similar way as cross-education of strength. In the “cross-activation” model, it is proposed that performing unilateral resistance training could induce bilateral cortical activation, potentially leading to concurrent neural adaptations in both trained and untrained hemispheres [ 50 , 52 , 53 , 54 , 55 ]. For example, it was previously found that unilateral resistance training increased corticospinal excitability in both the trained and untrained primary motor cortex [ 55 ]. Furthermore, decreases in interhemispheric inhibition [ 56 ], short-interval intracortical inhibition [ 52 , 57 ], and cortical silent period [ 58 , 59 ] were also observed in both the trained and untrained side following unilateral resistance training. However, whether or not these neural adaptations can explain the cross-education of muscular endurance is currently not known, and further research is needed.
4.3.3 Increase in Tolerance to Exercise-Induced Discomfort
Increases in tolerance to exercise-induced discomfort may in part play a role in the cross-education of muscular endurance. For example, previous studies have suggested that the cross-education of muscular endurance may be due to repeated exposures to uncomfortable exertions during a training intervention, which allows individuals to accommodate greater exercise-induced discomfort, pain, and/or fatigue sensation [ 23 , 27 , 30 , 32 ]. Although it is not directly related to exercise-induced discomfort perception, previous cross-sectional studies have demonstrated that athletes typically have higher pain tolerance when compared with nonathlete control individuals [ 60 , 61 ]. In addition, increased pain tolerance has been observed following aerobic and combined (aerobic + resistance) exercise training in healthy young adults [ 62 ]. It has been proposed that the higher pain tolerance observed in trained individuals may be due to enhanced pain coping strategies, developed through repeated exposure to physical and psychological stress during exercise [ 60 , 63 ]. This is further supported by a previous study in which 6 weeks of high-intensity interval training increased not only ischemic pain tolerance but also exercise tolerance (i.e., time to exhaustion) when compared with volume-matched moderate-intensity continuous training [ 64 ]. In that study, it was suggested that the improvement in pain tolerance is likely due to repeated exposure to high metabolic stress and exercise-induced noxious stimuli, which might partly explain the improvement in exercise tolerance [ 64 ]. Based on these findings, it is possible that repeated exposure to discomfort from unilateral resistance training can lead to increased tolerance, resulting in increased muscular endurance in the contralateral untrained limb. This proposed mechanism is unlikely to play a role in the cross-education of muscular endurance if the training intervention only induces very low levels of discomfort or pain (e.g., low repetition with low load). However, since this proposed mechanism is based on a study that implemented aerobic training intervention, it needs to be further examined with resistance training intervention.
4.4 Future Considerations
There has been extensive work on the cross-education of strength, but far less attention has been paid to the cross-education of muscular endurance. For example, there is a lack of randomized controlled studies, which makes it difficult to draw clear conclusions on the cross-education of muscular endurance. The inclusion of a time-matched nonexercise control group allows researchers to confidently conclude that the increase in muscular endurance in the untrained limb is due to the unilateral resistance training and not to some other factor. Thus, time-matched control groups are always recommended for future studies. In addition, it is common to see studies reporting within-group changes (i.e., pre- to posttest) for each training and control group, and when significant changes are observed only in the training group and not in the control group, it is often concluded that there is cross-education of muscular endurance. However, this interpretation is problematic since the change scores are not directly compared between groups (e.g., intervention group versus control group). In other words, it is important to test the group × time interaction or directly compare the change scores between the groups if the goal is to examine whether the changes in muscular endurance in the untrained limb differ between the groups [ 65 , 66 , 67 ].
Several included studies in the present review did not clearly indicate how they measured the cross-education of muscular endurance. For example, a number of studies measured the maximal number of repetitions using a certain percentage of maximum strength (e.g., 30% of 1RM); however, they did not clearly indicate whether an absolute or relative load/intensity was utilized at posttesting. This lack of clarity makes it difficult to compare results across the literature and to replicate the data in future works. Therefore, future studies should clearly state within their methodology whether muscular endurance was measured via an absolute or relative muscular endurance test. In addition to absolute/relative muscular endurance, several other types of outcome variables have been also examined to test muscular endurance (e.g., total work during a certain number of repetitions, time to task failure). This discrepancy in methodology may partially explain the inconsistent findings observed in the existing literature. At present, it remains unclear which outcome variable is the most appropriate way to test an individual’s muscular endurance, and thus further research is warranted. Of note, in the cross-education of strength literature, it has been suggested that the changes in strength in the contralateral untrained limb are the greatest when it is tested with the same movement task performed by the trained limb (training specificity; e.g., test and train dynamically) [ 4 ]. Based on this, it may be reasonable to test the cross-education of muscular endurance with the same movement task used for the training intervention. However, the question of whether the cross-education of muscular endurance follows the principle of specificity requires further investigation.
Future studies might examine other markers of endurance capacity (e.g., mitochondrial density, muscle capillarization) to provide better support for the idea that the mechanism underlying cross-education of muscular endurance may not be local per se, but potentially via neural adaptations. A final consideration for future studies, especially for those attempting to address potential underlying mechanisms, may be the use of mediation analysis. In the present review, we suggested a number of potential underlying mechanisms including changes in strength in the untrained limb (for absolute muscular endurance). In one of the included studies, for example, concurrent increases in strength and muscular endurance were observed in the untrained limb (i.e., cross-education of strength and muscular endurance) [ 23 ]. However, because there was concurrent cross-education of strength and absolute muscular endurance, this does not necessarily indicate that the cross-education of muscular endurance was driven by the cross-education of strength. One statistical approach to understanding the potential role of strength changes in cross-education of muscular endurance may be using a mediation analysis [ 46 , 47 ]. Mediation analysis can quantify the effect of the third (mediating) variable (e.g., changes in strength in untrained limb) on the relationship between the independent variable (e.g., intervention groups) and dependent variable (e.g., changes in absolute muscular endurance in untrained limb). This approach may help future studies with identifying the potential underlying mechanisms that contribute to the cross-education of muscular endurance (if it exists).
5 Conclusions
Performing unilateral resistance training has been shown to increase strength not only in the trained limb but also in the contralateral untrained limb (i.e., cross-education of strength). However, less attention has been paid to the question of whether performing unilateral resistance training can also increase muscular endurance in the contralateral untrained limb (i.e., cross-education of muscular endurance). The current body of the literature does not provide sufficient evidence to draw clear conclusions on whether a cross-education of muscular endurance is present. Therefore, further research with a nonexercise control group (i.e., randomized controlled trials) is necessary to draw a strong conclusion. Furthermore, some potential underlying mechanisms (i.e., increased strength, bilateral access model, increased tolerance) are discussed in the present review; however, the proposed ideas currently lack experimental evidence and require further research.
Schoenfeld BJ, Contreras B, Vigotsky AD, Peterson M. Differential effects of heavy versus moderate loads on measures of strength and hypertrophy in resistance-trained men. J Sports Sci Med. 2016;15(4):715.
PubMed PubMed Central Google Scholar
Jessee MB, Buckner SL, Mouser JG, Mattocks KT, Dankel SJ, Abe T, et al. Muscle adaptations to high-load training and very low-load training with and without blood flow restriction. Front Physiol. 2018;9(1448):1–11.
Google Scholar
Adams KJ, Swank AM, Berning JM, Sevene-Adams PG, Barnard KL, Shimp-Bowerman J. Progressive strength training in sedentary, older African American women. Med Sci Sports Exerc. 2001;33(9):1567–76.
Article CAS PubMed Google Scholar
Lee M, Carroll TJ. Cross education: possible mechanisms for the contralateral effects of unilateral resistance training. Sports Med. 2007;37(1):1–14.
Article PubMed Google Scholar
Manca A, Dragone D, Dvir Z, Deriu F. Cross-education of muscular strength following unilateral resistance training: a meta-analysis. Eur J Appl Physiol. 2017;117(11):2335–54.
Scripture EW, Smith TL, Brown EM. On the education of muscular control and power. Stud Yale Psychol Lab. 1894;2:114–9.
Carroll TJ, Herbert RD, Munn J, Lee M, Gandevia SC. Contralateral effects of unilateral strength training: evidence and possible mechanisms. J Appl Physiol. 2006;101(5):1514–22.
Manca A, Hortobágyi T, Rothwell J, Deriu F. Neurophysiological adaptations in the untrained side in conjunction with cross-education of muscle strength: a systematic review and meta-analysis. J Appl Physiol. 2018;124(6):1502–18.
Zhou S. Chronic neural adaptations to unilateral exercise: mechanisms of cross education. Exerc Sport Sci Rev. 2000;28(4):177–84.
CAS PubMed Google Scholar
Beyer KS, Fukuda DH, Boone CH, Wells AJ, Townsend JR, Jajtner AR, et al. Short-term unilateral resistance training results in cross education of strength without changes in muscle size, activation, or endocrine response. J Strength Condition Res. 2016;30(5):1213–23.
Article Google Scholar
Manca A, Hortobágyi T, Carroll TJ, Enoka RM, Farthing JP, Gandevia SC, et al. Contralateral effects of unilateral strength and skill training: modified Delphi consensus to establish key aspects of cross-education. Sports Med. 2021;51(1):11–20.
Bemben MG. Age-related alterations in muscular endurance. Sports Med. 1998;25:259–69.
Liguori G. American College of Sports Medicine. ACSM’s guidelines for exercise testing and prescription. Philadelphia: Lippincott Williams & Wilkins; 2020.
Fliss MD, Stevenson J, Mardan-Dezfouli S, Li DC, Mitchell CJ. Higher-and lower-load resistance exercise training induce load-specific local muscle endurance changes in young women: a randomised trial. Appl Physiol Nutr Metab. 2022;47(12):1143–59.
Waller G, Dolby M, Steele J, Fisher JP. A low caffeine dose improves maximal strength, but not relative muscular endurance in either heavier-or lighter-loads, or perceptions of effort or discomfort at task failure in females. PeerJ. 2020;8: e9144.
Article PubMed PubMed Central Google Scholar
Pincivero D, Lephart S, Karunakara R. Reliability and precision of isokinetic strength and muscular endurance for the quadriceps and hamstrings. Int J Sports Med. 1997;18(02):113–7.
Kon M, Ohiwa N, Honda A, Matsubayashi T, Ikeda T, Akimoto T, et al. Effects of systemic hypoxia on human muscular adaptations to resistance exercise training. Physiol Rep. 2014;2(6): e12033.
Chatlaong MA, Bentley JP, Buckner SL, Mattocks KT, Dankel SJ, Loenneke JP, et al. Mechanisms mediating increased endurance following high-and low-load training with and without blood flow restriction. J Trainol. 2022;11(1):7–11.
Groennebaek T, Jespersen NR, Jakobsgaard JE, Sieljacks P, Wang J, Rindom E, et al. Skeletal muscle mitochondrial protein synthesis and respiration increase with low-load blood flow restricted as well as high-load resistance training. Front Physiol. 2018;9:1796.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73.
Fariñas J, Rial-Vázquez J, Carballeira E, Giráldez-García MA, Colomer-Poveda D, Sevilla-Sánchez M, et al. Cross education is modulated by set configuration in knee extension exercise. J Musculoskelet Neuronal Interact. 2023;23(1):43.
Fariñas J, Mayo X, Giraldez-García MA, Carballeira E, Fernandez-Del-Olmo M, Rial-Vazquez J, et al. Set configuration in strength training programs modulates the cross education phenomenon. J Strength Condition Res. 2021;35(9):2414–20.
Ben Othman A, Behm DG, Chaouachi A. Evidence of homologous and heterologous effects after unilateral leg training in youth. Appl Physiol Nutr Metab. 2018;43(3):282–91.
Kannus P, Alosa D, Cook L, Johnson RJ, Renström P, Pope M, et al. Effect of one-legged exercise on the strength, power and endurance of the contralateral leg. Eur J Appl Physiol Occup Physiol. 1992;64(2):117–26.
Shaver LG. Muscular endurance in ipsilateral and contralateral arms: influence of training and inactivity. Arch Phys Med Rehabil. 1973;54(11):505–10.
Shaver LG. Cross transfer effects of training and detraining on relative muscular endurance. Am Correct Ther J. 1973;27(2):49–50.
Shaver LG. Effects of training on relative muscular endurance in ipsilateral and contralateral arms. Med Sci Sports. 1970;2(3):165–71.
Meyers CR. Effects of two isometric routines on strength, size, and endurance in exercised and nonexercised arms. Res Q Am Assoc Health Phys Educ Recreat. 1967;38(3):430–40.
CAS Google Scholar
Kruse RD, Mathews DK. Bilateral effects of unilateral exercise: experimental study based on 120 subjects. Arch Phys Med Rehabil. 1958;39(6):371–6.
Slater-Hammel AT. Bilateral effects of muscle activity. Res Q Am Assoc Health Phys Educ Recreat. 1950;21(3):203–9.
Hedayatpour N, Golestani A, Izanloo Z, Meghdadi M. Unilateral leg resistance training improves time to task failure of the contralateral untrained leg. Acta Gymn. 2017;47(2):72–7.
Yuza N, Ishida K, Miyamura M. Cross transfer effects of muscular endurance during training and detraining. J Sports Med Phys Fitness. 2000;40(2):110.
Pincivero DM, Lephart SM, Karunakara RG. Effects of rest interval on isokinetic strength and functional performance after short-term high intensity training. Br J Sports Med. 1997;31(3):229–34.
Article CAS PubMed PubMed Central Google Scholar
Sinoway L, Shenberger J, Leaman G, Zelis R, Gray K, Baily R, et al. Forearm training attenuates sympathetic responses to prolonged rhythmic forearm exercise. J Appl Physiol. 1996;81(4):1778–84.
Grimby G, Aniansson A, Hedberg M, Henning G, Grangard U, Kvist H. Training can improve muscle strength and endurance in 78-to 84-yr-old men. J Appl Physiol. 1992;73(6):2517–23.
Parker R. The effects of mild one-legged isometric or dynamic training. Eur J Appl Physiol. 1985;54:262–8.
Article CAS Google Scholar
Tesch P, Karlsson J. Effects of exhaustive, isometric training on lactate accumulation in different muscle fiber types. Int J Sports Med. 1984;5(02):89–91.
Yasuda Y, Miyamura M. Cross transfer effects of muscular training on blood flow in the ipsilateral and contralateral forearms. Eur J Appl Physiol. 1983;51(3):321–9.
Hodgkins J. Influence of unilateral endurance training on contralateral limb. J Appl Physiol. 1961;16(6):991–3.
Walters CE, Stewart CL, LeClaire JF. Effect of short bouts of isometric and isotonic contractions on muscular strength and endurance. Am J Phys Med Rehabil. 1960;39(3):131–41.
Mathews DK, Shay CT, Godin F, Hogdon R. Cross transfer effects of training on strength and endurance. Res Q Am Assoc Health Phys Educ Recreat. 1956;27(2):206–12.
Porter C, Reidy PT, Bhattarai N, Sidossis LS, Rasmussen BB. Resistance exercise training alters mitochondrial function in human skeletal muscle. Med Sci Sports Exerc. 2015;47(9):1922.
Groennebaek T, Vissing K. Impact of resistance training on skeletal muscle mitochondrial biogenesis, content, and function. Front Physiol. 2017;8:713.
Henneman E, Somjen G, Carpenter DO. Excitability and inhibitibility of motoneurons of different sizes. J Neurophysiol. 1965;28(3):599–620.
Ploutz LL, Tesch PA, Biro RL, Dudley GA. Effect of resistance training on muscle use during exercise. J Appl Physiol. 1994;76(4):1675–81.
Hayes AF, Preacher KJ. Statistical mediation analysis with a multicategorical independent variable. Br J Math Stat Psychol. 2014;67(3):451–70.
Hayes AF, Rockwood NJ. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav Res Ther. 2017;98:39–57.
Colomer-Poveda D, Romero-Arenas S, Fariñas J, Iglesias-Soler E, Hortobágyi T, Márquez G. Training load but not fatigue affects cross-education of maximal voluntary force. Scand J Med Sci Sports. 2021;31(2):313–24.
Wong V, Spitz RW, Song JS, Yamada Y, Kataoka R, Hammert WB, et al. Blood flow restriction augments the cross-education effect of isometric handgrip training. Eur J Appl Physiol. 2024;124:1575–85.
Ruddy KL, Carson RG. Neural pathways mediating cross education of motor function. Front Hum Neurosci. 2013;7:1–22.
Lee M, Hinder MR, Gandevia SC, Carroll TJ. The ipsilateral motor cortex contributes to cross-limb transfer of performance gains after ballistic motor practice. J Physiol. 2010;588(1):201–12.
Kidgell DJ, Frazer AK, Rantalainen T, Ruotsalainen I, Ahtiainen J, Avela J, et al. Increased cross-education of muscle strength and reduced corticospinal inhibition following eccentric strength training. Neuroscience. 2015;300(June):566–75.
Colomer-Poveda D, Romero-Arenas S, Keller M, Hortobágyi T, Márquez G. Effects of acute and chronic unilateral resistance training variables on ipsilateral motor cortical excitability and cross-education: a systematic review. Phys Ther Sport. 2019;40:143–52.
Frazer AK, Williams J, Spittle M, Kidgell DJ. Cross-education of muscular strength is facilitated by homeostatic plasticity. Eur J Appl Physiol. 2017;117(4):665–77.
Mason J, Frazer AK, Horvath DM, Pearce AJ, Avela J, Howatson G, et al. Ipsilateral corticomotor responses are confined to the homologous muscle following cross-education of muscular strength. Appl Physiol Nutr Metab. 2018;43(1):11–22.
Hortobágyi T, Richardson SP, Lomarev M, Shamim E, Meunier S, Russman H, et al. Interhemispheric plasticity in humans. Med Sci Sports Exerc. 2011;43(7):1188–99.
Goodwill AM, Pearce AJ, Kidgell DJ. Corticomotor plasticity following unilateral strength training. Muscle Nerve. 2012;46(3):384–93.
Latella C, Kidgell DJ, Pearce AJ. Reduction in corticospinal inhibition in the trained and untrained limb following unilateral leg strength training. Eur J Appl Physiol. 2012;112(8):3097–107.
Coombs TA, Frazer AK, Horvath DM, Pearce AJ, Howatson G, Kidgell DJ. Cross-education of wrist extensor strength is not influenced by non-dominant training in right-handers. Eur J Appl Physiol. 2016;116(9):1757–69.
Tesarz J, Schuster AK, Hartmann M, Gerhardt A, Eich W. Pain perception in athletes compared to normally active controls: a systematic review with meta-analysis. Pain. 2012;153(6):1253–62.
Johnson MH, Stewart J, Humphries SA, Chamove AS. Marathon runners’ reaction to potassium iontophoretic experimental pain: pain tolerance, pain threshold, coping and self-efficacy. Eur J Pain. 2012;16(5):767–74.
Anshel MH, Russell KG. Effect of aerobic and strength training on pain tolerance, pain appraisal and mood of unfit males as a function of pain location. J Sports Sci. 1994;12(6):535–47.
Song JS, Yamada Y, Kataoka R, Wong V, Spitz RW, Bell ZW, et al. Training-induced hypoalgesia and its potential underlying mechanisms. Neurosci Biobehav Rev. 2022;141: 104858.
O’Leary TJ, Collett J, Howells K, Morris MG. High but not moderate-intensity endurance training increases pain tolerance: a randomised trial. Eur J Appl Physiol. 2017;117(11):2201–10.
Dankel SJ. Simple ways to make the results of exercise science studies more informative. J Trainol. 2020;9(2):43–9.
Huck SW, McLean RA. Using a repeated measures ANOVA to analyze the data from a pretest-posttest design: a potentially confusing task. Psychol Bull. 1975;82(4):511–8.
Maxwell SE, Howard GS. Change scores—necessarily anathema? Educ Psychol Meas. 1981;41(3):747–56.
Download references
Acknowledgements
Author information, authors and affiliations.
Department of Health, Exercise Science, and Recreation Management, Kevser Ermin Applied Physiology Laboratory, The University of Mississippi, P.O. Box 1848, University, MS, 38677, USA
Jun Seob Song, Yujiro Yamada, Ryo Kataoka, William B. Hammert, Anna Kang & Jeremy P. Loenneke
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Jeremy P. Loenneke .
Ethics declarations
No sources of funding were used to assist in the conduct of this review or the preparation of this article.
Conflict of Interest
The authors declare that they have no conflicts of interest relevant to the content of this article.
Ethics Approval
Not applicable.
Consent to Participate
Consent for publication, availability of data and material.
Available upon request from the corresponding author.
Code Availability
Author contributions.
JSS carried out the systematic scoping review. YY, RK, WBH, AK, and JPL contributed to the manuscript writing. All authors have read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Song, J.S., Yamada, Y., Kataoka, R. et al. Cross-Education of Muscular Endurance: A Scoping Review. Sports Med (2024). https://doi.org/10.1007/s40279-024-02042-z
Download citation
Accepted : 30 April 2024
Published : 17 May 2024
DOI : https://doi.org/10.1007/s40279-024-02042-z
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Find a journal
- Publish with us
- Track your research
IMAGES
VIDEO
COMMENTS
Inclusive Education: A Literature Review on Definitions, Attitudes and Pedagogical Challenges. April 2021. International Journal of Research and Innovation in Social Science V (III):358-365. DOI ...
Inclusive education focuses on students with disabilities and every student; it also focuses on educational policies and organisations. ... System theory is sometimes used in research on inclusive education. For example, ... a Bibliometric Review of the Literature Over 25 Years." International Journal of Inclusive Education, 1-20. doi:10. ...
Elaborated theory. Whereas, research about, for example, the attitudes to and effectiveness of inclusive education has been largely concerned with relationships between variables, there is a lot of research into inclusive education that has been grounded in very elaborated theories (cf. e.g. Allan Citation 2008).Skrtic (Citation 1991, Citation 1995) is an example of an early theorist who has ...
A systematic literature review was conducted to identify studies focused on interventions aiming to improve inclusive education in low- and lower-middle-income countries. The searches returned 1,266 studies for a title and abstract review. Only 31 studies evaluated interventions and included 20 or more respondents.
In the academic literature, inclusive education is presented as an ideology (Allan 2014) that guides practice to respect the right of all learners to quality education.Booth noted that inclusive education focuses on increasing participation for all learners, creating systems that value all individuals equally, and promoting equity, compassion, human rights, and respect.
Inclusive education is not just a goal; it is a commitment to making sure that every student, regardless of their unique needs, can learn, grow, and thrive in a diverse classroom. However, as we explore the world of inclusive practices, it becomes evident that there are challenges to overcome, but also innovative solutions to celebrate. ...
By promoting social inclusion, inclusive education better prepares learners for adult life. The literature defines social inclusion as a set of dimensions that are relevant to individual characteristics, relationships and social networks, active enrolment in school, employment, living in the community, and so on.
Introduction. Evident from international laws, inclusive education (IE) is globally recognized as instrumental in facilitating equity and quality education for all students (Alquraini & Gut, 2012; Romero-Contreras, Garcia-Cedillo, Forlin, & Lomelí-Hernández, 2013).For example, the Salamanca Statement (UNESCO, 1994) contends that IE is "the most effective means of combating discriminatory ...
Keywords: inclusive education; equity, review; inclusion Changing ideas on inclusive education For inclusive education to be at the core of education—as it should be—it has to be a truly inclusive education, not one that is narrowly defined. It can be so, and there has certainly been a progressively broadening compass to the idea of inclu
We conducted a critical systematic literature review on global inclusive education and law. The critical review questions were: (1) how have scholars theorized, conceptualized, and studied global inclusive education? (2) How do scholars define global inclusive education? (3) And what do scholars cite as prominent international inclusive education law? We ask such questions given the ongoing ...
This paper on inclusive education explores several diverse viewpoints from various scholars in different contexts on the concepts of inclusive education in an effort to reach the common understanding of the same this concept. The attitudes section is addressed from the perspectives of pupils, educators, and the society (parents), and it further explore the dilemmas that teachers and students ...
Abstract: This paper on inclusive education explores several diverse viewpoints from various scholars in different contexts on the concepts of inclusive education in an effort to reach the common understanding of the same this concept.
This systematic literature review 'speaks to' and builds on two previous literature reviews: ... Nine journals were represented by a single paper—the only exception was the International Journal of Inclusive Education with four articles. The range of journals also reflects the different approaches to inclusive pedagogies discussed later ...
This systematic literature review could focus on only a small amount of literature on inclusive teaching practices in self-proclaimed inclusive education settings. Asserting that the educational setting was within the scope of inclusion by studies and authors is one of the major limitations within the narrative synthesis.
Inclusive Education, as one of the scholarly concepts, appears to lack a globally agreed meaning even though attempts have been made across vast literature. According to Shyman (2015) capturing the concept IE as both an educational principle and. a practical application is far more than intellectually challenging.
Inclusive Education: Literature Review. Professor Dillip Giri. The education of disabled children never received such amount of consideration and special efforts by government and non-government agencies in past as in present days. The attitude of the community in general and the attitude of parents in particular towards the education of the ...
review of the literature on inclusive education in the English- and Spanish-language litera-ture (Amor et al, 2018). Amor et al. (2018) reviewed all articles published between 2002 and 2016 on inclusive education and adopted a definition of inclusion that was used to guide the overall search: inclusion is when students
This brief review of relevant literature on inclusive education forms a component of the larger Inclusive School Communities Project: Final Evaluation Report delivered by the Research in Inclusive and Specialised Education (RISE) team to JFA Purple Orange in October, 2020. Suggested citation for full evaluation report:
Example of a Literature Review on General Educators' Perceptions of Inclusion By Kimberly Rombach Consider the following general education teacher's description of being notified that she will be teaching students with disabilities in the near future: They [the administration] put a note in my mailbox in June telling me I
Background The current paradigm of competency-based medical education and learner-centredness requires learners to take an active role in their training. However, deliberate and planned continual assessment and performance improvement is hindered by the fragmented nature of many medical training programs. Attempts to bridge this continuity gap between supervision and feedback through learner ...
Facing long-standing barriers for effective comprehensive education, secondary schools show specific interests, strengths and needs in a school-wide movement towards inclusion. Reviewing literature of recent research in inclusion in secondary schools (2000-2012), current interests represent inclusive culture, policy and practices, although ...
Review of the literature identified that no existing survey was available for use with nursing students in the Canadian context. However, an analysis of themes across qualitative and quantitative studies of physicians, medical students, nurses, and nursing students provided sufficient data to develop a preliminary set of items suitable for ...
A scoping review was conducted to evaluate the cross-education of muscular endurance. The current study was conducted and reported in accordance with the Preferred Reporting for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) [].To identify relevant articles for the current scoping review, systematic literature searches were conducted from inception through ...
The 'novel perspective' is a complexity theory approach to the development of inclusive education in South Africa. Our research process commenced with an overview of South African laws, policy documents and official reports and of published scholarly literature on special and or inclusive education from 1948 to 2021.